
Your bowel function is vital for living a healthy life, but how much do you know about how it works?
My Amazing Body is a podcast where we explore interesting, unknown and misunderstood parts of your body with help from medical experts and stories from real Queenslanders.
This episode is all about your bowel. What does your bowel do, where is it and what does it look like? Is it all about poo? General and colorectal surgeon Dr Ming Ho explains how the bowel works, and the types of conditions that can affect bowel health. Queensland woman Kate talks about her experience with Crohn’s disease, a type of inflammatory bowel disease.
Meet our guests


Episode materials
Audio is great, but some things are best seen as well as heard, or might tempt you to do further reading. These materials provide more information about topics we touch on in the show.
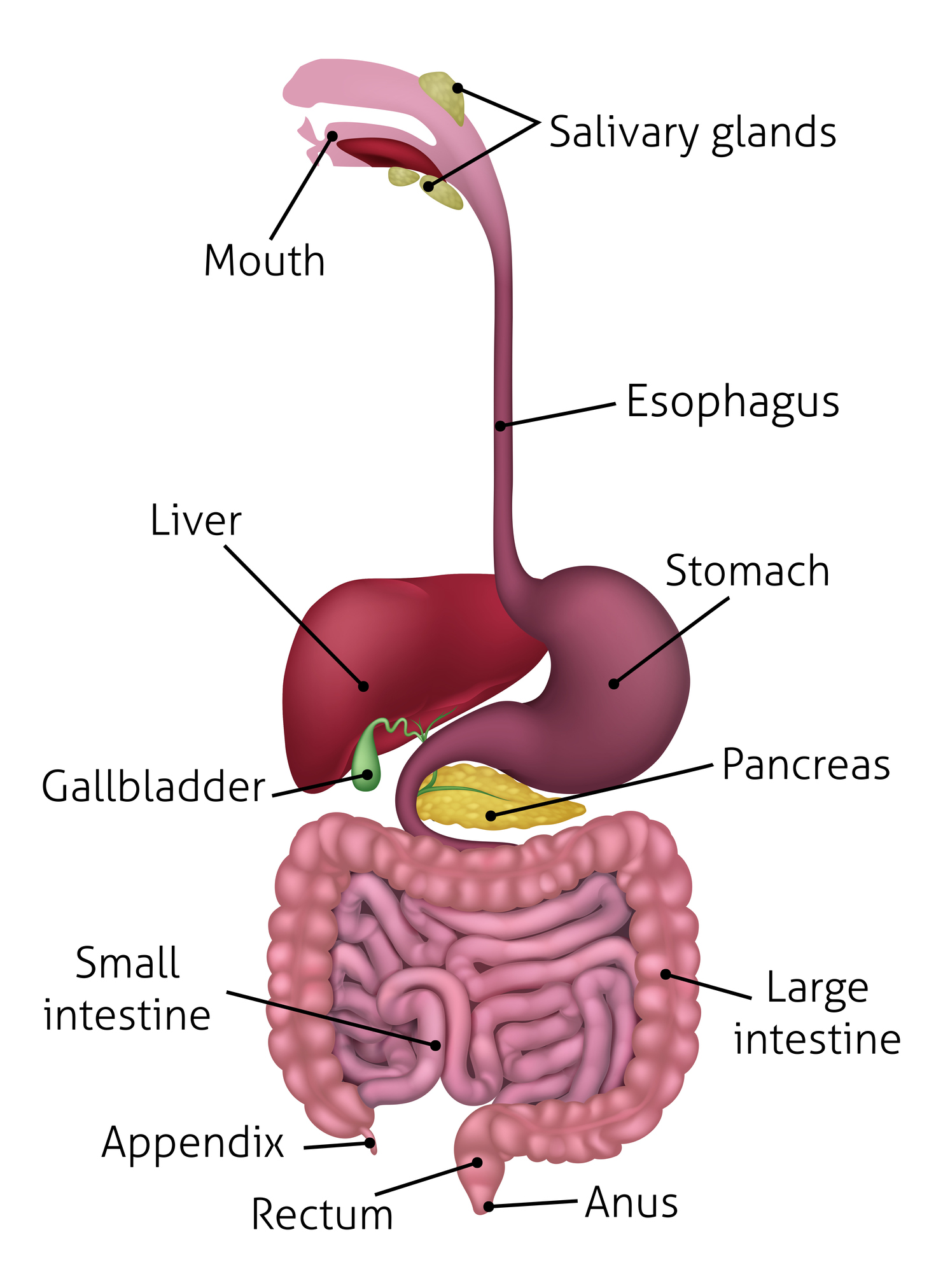
The bowel
The National Bowel Cancer Screening Program
If you’re aged 50 or over, you’ll receive a free bowel cancer testing kit in the mail as part of the National Bowel Cancer Screening Program. You can find more information about this program at the National Bowel Cancer Screening Program website.
Bowel cancer prevention
Dr Ming Ho explains that a lot of his work revolves around testing for and treating bowel cancer. You can find more information about bowel cancer prevention at the links below.
National Bowel Cancer Screening Program
Crohn’s disease
Inflammatory bowel diseases, like Crohn’s disease or ulcerative colitis, affect almost 75,000 Australians. In this episode, Kate shares her story of being diagnosed with and living with Crohn’s disease.


You can find more information about these diseases at the links below.
Health Direct: Crohn’s disease
Health Direct: Ulcerative colitis
Transcript
Dr Ming Ho: When you look at it, it is alive. It got its own nervous supply. It got its own nervous system, which is independent from the rest of your body. So, it's almost like a whole bag of worms that very slowly moving along, which is fascinating.
Host: That is Rockhampton Hospital general and colorectal surgeon, Dr Ming Ho. Believe it or not, he's talking about what your bowel would look like if he was operating on you.
Dr Ming Ho: How interesting we do operation when people are having a general anaesthesia, so they are asleep and they have the various medication to paralyse them, so they do not move. That's how we can operate on them. But despite the fact that you're fully paralysed during the operation, your bowels continue to move, continue to work.
Host: Welcome to this episode of My Amazing Body, a podcast where we explore interesting, unknown and misunderstood parts of your body. Today, we're learning all about your bowel.
What is your bowel and what does it do? Is it all about making poo? Well, Dr Ming Ho explains that for a start, the word bowel is actually a collective term for a number of different parts of your body that do a number of different things.
Dr Ming Ho: People mention the word bowel, but that can mean a lot of things. In our area, the bowel is the end of the digestive tract, so after the food goes to the mouth, goes down to your food pipe, gets down to your stomach, after that, it enters into the bowel. So, the bowel is divided into large bowel and small bowel. The first part after the stomach, it's the small bowel. What it does is further digest the food that you eat and absorb the food that you eat. And after digestion, the food material will generally break down into another part of the food and enter your large bowel. Your large bowel will regulate the food content, the water within the stuff that you eat, and absorb it. At the very end, it becomes waste. The large bowel also stores up the waste, and when you’re in the socially acceptable situation, you carry off the waste. So, it is very important, you can't live without it.
It's also known as the small intestine, and the large bowel also known as the large intestine or colon, some people will also refer that to as well.
Host: The bowel is an amazing organ. As we heard Dr Ming Ho describe, it moves by itself, and it can also stretch and bend as you eat and drink throughout the day.
Dr Ming Ho: The bowel is a very elastic organ. So, in terms of small bowel, it can stretch up to a good few metres. And when it's not being used, it’s very tiny. So, I would say, like the width of your ballpoint pen. It lies almost like a bit like noodles. So, when it's working, it’s got food in it, it can dilate up to a few centimetres. So, for example, if someone has a bowel obstruction, the small bowel can dilate up to maybe five, six centimetres; it's not unusual. So, you've got a very flexible tissue. That's why you can accommodate the different conditions, when you're starving or when you're fully fed.
Host: Parts of your bowel are also home to trillions of bacteria. Study of what these tiny organisms are doing in your body is ongoing, but Dr Ming Ho says we know enough to know they're very important.
Dr Ming Ho: There's a lot of bacteria in the bowel and it depends which part of the bowel you're talking about. Mainly in the proximal small bowel, there shouldn't be any bacteria. Your stomach should kill it all. But we do know it now that a few strains of bacteria can live within the acid, like H. pylori, they can live in the stomach despite the fact that there’s a lot of acid in there. The small bowel itself generally is sterile, but when you get down to the distal small bowel and down to the large bowel, the bacteria start growing, and there's a very complex relationship between the bacteria and also to the host, which is you.
The interaction is actually very important to maintain the health of the bowel and also your health. Just an interesting fact, for example, when you're talking about faecal matter; know that maybe two-thirds of the faecal matter is actually made from bacteria. So, you are what you eat, but you are not only you, you are actually living with a whole big community within your bowel, which is a whole complex relationship they create from the bacteria within you.
Host: If you're keen on learning more about the bacteria that live in your gut, check out episode 4 in season one of My Amazing Body - it's all about your gut microbiome.
Dr Ming Ho is a colorectal surgeon, which means if he's working on your bowel, it's probably because something's not quite right with it. We asked him about some of the common conditions that affect the bowel.
Dr Ming Ho: For colonic disease, one of the big things to emphasis, or two big emphases that we have, are prevention of cancers. A large majority of my work is for cancer prevention and treatment. Bowel cancer is one of the most common cancers that we have in Australia. And as you know, our government sponsored a very large bowel screening program, and a lot of our work actually devoted into that, so i.e., managing the colonoscopy.
Host: The program Dr Ming Ho is referring to is the National Bowel Cancer Screening Program.
Each year, people aged 50 to 74 across Australia are sent a free bowel cancer screening kit in the mail. If their sample comes back with any indication, they could have cancer, they'll be referred to a specialist like Dr Ming Ho for a colonoscopy.
Dr Ming Ho: So, once you turn the age of 50, you will get a pack from the government called FOBT, it is your faecal occult blood test kit. You just need to send a sample of your poo into the kit, send it back to the government and they will process it.
What it does is to look for any blood that's not visible to naked eye, which is very often the first sign for people having bowel cancer or any significant polyp, which is a protrusion of tissue before they turn into cancer. So then if you’ve got any blood into that poo test, then you will need a colonoscopy to check it out. So, it's very important to get a screening and get a colonoscopy as appropriate. So, this is a screening test, and for the people who have any kind of bowel symptom, particularly after the age of 50, they need to talk to your local doctor and get referred to a surgeon or gastroenterology to discuss whether they need a colonoscopy. So, this is the most important preventative things that we can offer to avoid you getting cancer or to treat your early diagnosis of cancer, which is a very, very treatable disease at the early stage.
Host: As well as regularly participating in screening, Dr Ming Ho stresses that some of the most important things you can do to protect your bowel health start before you ever need to see a surgeon.
Dr Ming Ho: So, the most important thing is prevention. Involve yourself in regular exercise, eat a healthy diet, don't smoke, and have a good lifestyle. Don't get too stressed and maintain your health. And this is the best thing that you can do to prevent having any kind of cancer, essentially, because you cannot control your genes.
Host: You can find more information about the program and how it works on the National Bowel Cancer Screening Program website, which we've linked to in our shownotes.
Are you enjoying this season of My Amazing Body? If you like it, why not tell others by leaving a rating or review in your podcast app or sharing that you're listening on socials. We know people love a personal recommendation, so please, spread the word!
Are you ready for this episode's mystery body part? See if you can guess the body part from the clues given. We'll reveal the answer at the end of the episode.
I didn't always exist, but once I'm with you, I'm with you for life.
Most people don't clean me much, which means I am full of bacteria - you can't see them, but you can see me!
If you're scared of seeing me, or having me touched, you have omphalophobia.
Do you know what I am?
Another reason you might see a surgeon like Dr Ming Ho for a bowel problem is if you have bowel obstruction. This is an emergency condition that happens when your bowel gets blocked up with poo that you can't get out, causing pain, loss of appetite, nausea and vomiting.
Dr Ming Ho: So, when people have a bowel obstruction it’s at the point that the blood supply to the bowel is being compromised by the pressure generated from the content within the bowel. So, the blood supply being cut off and that part of the bowel will die. And then eventually you perforate and end up with a condition called peritonitis, potentially lethal and you need an emergency operation.
Host: Your bowel can get blocked up for a number of reasons: untreated constipation, a medical condition like irritable bowel syndrome, or even the bowel twisting shut on itself. If you think you might have an impacted bowel, you should see your doctor immediately.
Dr Ming Ho also treats Queenslanders with rarer bowel conditions, including inflammatory bowel diseases.
Dr Ming Ho: The other part of our work is for benign disease of the colon. That’s what we call inflammatory bowel disease. They're not as common, but they are a group of chronic disease that actually need a lot of attention and care. So, they actually take up a lot of our time.
Host: One type of inflammatory bowel disease is called Crohn's disease. Named after a gastroenterologist called Dr Burrill Crohn, who worked in the team that discovered it in 1932, the main characteristic of Crohn's is inflammation in the bowel caused by the immune system. It can be very painful and cause chronic diarrhoea, fatigue, reduced appetite and weight loss. Dr Ming Ho says that after all this time, the disease is still a bit of a mystery.
Dr Ming Ho: So, we know that it is a disease that has some partial genetic causes. We know it in the monozygotic twins, if one has Crohn's, the other has a very high incidence of getting Crohn's disease. But the environmental factors often actually have interplay with them. We know that the diet will affect the degree of inflammation within the bowel, which is a hallmark of the Crohn's disease. So, it is like a multifactorial disease with a lot of factors on the plate. The onset is very insidious. It very commonly happens when people have this vague abdominal pain undiagnosed of anything.
Host: We spoke with Queensland woman Kate, who was diagnosed with Crohn's disease a few years ago, about her experience with the condition.
Kate: It was when I first moved to a small rural town up in Far North Queensland, which was Weipa, and I was on a single person villa campsite in the mines. And I started getting a bit of a fever, and it felt like I was getting food poisoned. A lot of diarrhea, just unwell, a bit of fatigue. And I brushed it aside thinking it might've been food poisoning from the new work environment.
Host: But it wasn't food poisoning. Kate's bouts of sickness continued over the coming months. She was tested for other illnesses like Giardia but got negative results. It wasn't until her doctor did test to check for inflammation in her bowel that they started to home in on the problem.
Kate: And after that, it didn't really improve, and it wasn't until I got an inflammation marker from my GP and the results came back that I was very likely to have inflammation in my bowel, the inflammation marker was very high, and it was very fortunate that a gastroenterologists was coming up that next week to the town, because he would visit every three months. And I had my colonoscopy and was diagnosed with Crohn's disease.
Host: Dr Ming Ho says that because the disease is a bit of a mystery and because the symptoms look a lot like other, more common conditions, it can be the case that patients like Kate have a lot of different tests done before they get a diagnosis, even though she's actually a typical Crohn's patient.
Dr Ming Ho: So multiple trips to the local doctors, even to the emergency, to have investigations, and even with a colonoscopy, they can't actually find a cause. It’s more common in ladies. And so, when you said that you got a young lady suffer from Crohn's, it's almost like a classical patient.
Host: After her inflammation markers came back so high, Kate had a colonoscopy to check for inflammation that would signal she had Crohn's.
Kate: So, after I was diagnosed with Crohn's, because the colonoscopy, when they went in, they only went through the large bowel, and they usually can stick their head through and see the small bowel as well. However, I was so inflamed, they couldn't actually see how far it went up in my small bowel. So, they put me on a dose of steroids, hoping that the inflammation would subside. However, my symptoms of diarrhea and cramping and just general fatigue didn't subside.
So I was sent down to Cairns and had an MRI, and in the MRI it showed that it wasn't just the inflammation, it actually had strictured, which is basically inflammation that is no longer elastic, and the steroid won't reduce the inflammation. It's kind of scarred there. So, the only way to get rid of that scarring is to cut it out.
Host: While she waited for surgery, Kate was on a liquid diet because her bowel couldn't pass any more solid food, and she took supplements to try and maintain some body weight. After a month, she travelled to Brisbane for an operation called a hemicolectomy to remove the damaged part of her bowel.
Kate: Hemicolectomy means partial, and colectomy means bit of intestine cut out. So, I had that. I had about 40 centimetres cut out, which might seem like a lot, but then you've got a lot of bowels. So, I still got enough. And I had my surgery, and I just remember waking up, and it actually went longer than anticipated. I had a fistula, which is when some of your intestine is connected to your bladder, or any kind of other organ, and mine was the urinary tract, so that took a bit more time.
Host: Kate found her first hours and days of recovery to be painful and a bit frightening!
Kate: So, I came out quite late, and all I remember is when I first woke up in the recovery room, was just a lot of pain, and they must've given me more morphine, but I just went in and out of consciousness. The first night was definitely the hardest, I had no idea what to expect. I remember waking up and hearing all this beeping and thinking, oh my God, code blue, I'm going to die, all this beeping. But it's just the normal lines and devices around me that were just beeping. So that was a bit scary.
Host: As Kate recovered from her surgery, she was encouraged to start eating solid foods to get her bowel working normally again.
Kate: So, after surgery they encourage solid food intake straight away. I wasn't allowed to be discharged from hospital until I had my first bowel movement, which is quite difficult when you have your pain medication, because morphine side effect is constipation. So, it's really balancing that fact of less pain meds to allow your bowel movement to start. So, yeah, I started straight away. I think I had rice bubbles the next day. I had no appetite at that moment, but you do what you got to do.
Host: While surgery is often a necessary treatment, Dr Ming Ho explains that an operation to cut out the disease isn't a cure-all for a condition like Crohn's.
Dr Ming Ho: The principle of a surgery is to preserve the bowel. We know that people who need surgery for Crohn's disease have very high chance to need the second or third surgery to repair further. So every time we will remove some bowel, and after three or four surgeries the patient may run out of bowel and then end up a condition called a short bowel syndrome, which means that you haven't actually got enough bowel left to perform the vital function, to sustain your life. So, you can't actually absorb adequate nutrients, which is a life-threatening situation. So, for surgery, we try to get the patient out of trouble, and then we will hand it over. We'll work with our gastroenterology colleagues; they can give the different kinds of medication to control disease. We actually haven't got a cure for Crohn's, but it can be managed in the majority of the time.
Host: For Kate, this was true; surgery didn't cure her condition.
Kate: About six months you have a postop colonoscopy check-up, and during that check-up, there was some inflammation starting to appear at the site where that had been removed. So, I did start on some treatment, that I didn't actually respond very well to it. Being very isolated in a rural town, it was hard to get the proper monitoring of the drug that I was on. However, I have changed medication and have followed some treatment from the Center of Digestive Diseases down in Sydney, and I'm actually doing really well at the moment. I'm pretty much in remission at the moment. I've got no inflammation there, so at the moment things are going really well.
Host: Crohn's is a relapsing and remitting disease, which means it can come back throughout life. But, it can be managed, and Kate shared with us how she's found balance in looking after her bowel over time.
Kate: I guess when you go through these kinds of big life changes or surgery, or get diagnosed with something, you kind of clutch on to anything that you can control. So for me, the things that I could control was what I put in my body, the sleep that I got, the exercise I was doing, just trying to live my most healthy life. But it also comes to a point where there's a certain... It's all on a spectrum. You can be very, very strict with to make sure that you do nothing wrong, and then you can be really relaxed. And I find that if you are very, very strict, you can have more stresses related to trying to eat the perfect diet for your condition. But the stress that goes through that may kind of unbalanced it out. So at the moment, I'm just eating as healthy as I can be, but not really worrying.
Host: We all know that talking about poo and pain can be a little uncomfortable. But Kate urges others who are experiencing any bowel issues at all to see their doctor, so they can find out what's going on.
Kate: I think you know your body better than anyone else, and if you think something's not right, I'd definitely go and see a professional and explain your symptoms.
But before doing that, the best thing to do is to make your own diary and date and time different things. So, if you're going to the toilet two times a day, pretty regularly, and then all of a sudden, your bowel movements increased to about six and they're more loose consistency, or you're getting more cramps. The best thing to do, if you're a bit embarrassed or you don't want to go and see a GP straight away, is to just record that down, because that's really important data for the GP to make that diagnosis. It could just be food poisoning, or it could be something more sinister.
I definitely think that you shouldn't be embarrassed talking about those things, that's what our health professionals are there for. They've seen and heard all those wonderful stories, and poo stories, so it shouldn't be embarrassing. It's all confidential, and you don't want to sweep something under the rug you wait too long and you need surgery. So, I definitely think you know when something's not right, and take that initiative and go and see your doctor.
Host: In fact, Kate's experience with her bowel condition has only made her want to learn more about it, and she's now embarking on a career change into medicine.
Kate: I am actually an engineer, but after being diagnosed with Crohn's and realizing that I'm so interested in the bowel, and just having that personal relationship, or not personal, but just interacting with patients and stuff like that and how important my surgeon was to me, I've actually gone back to university and I've actually got into medicine. So, I'm a second-year medical student at the moment. And I'm very interested in hopefully one day maybe becoming a gastroenterologist or something in the field that I can share my experience, but also help in a more professional way.
Host: In his role as both a general and colorectal surgeon, Dr Ming Ho does all sorts of surgeries, and it's clear he's pretty passionate about his job.
Dr Ming Ho: I think my most favourite part of the job is, I actually like the emergency colonic surgery. So, when people are having this emergency it’s one of the worst feelings the patient can have. And one of my jobs I can do is get them out of it. So, after a surgery, we clean it up and they go home in three, four days' time as a new person. I think there's nothing really more rewarding than that. So, they come in in impending doom, almost dying, and they walk out the hospital in around three, four days' time and go back to normal life. I think this is the most satisfying moment of my life.
Host: Thanks for listening to this episode of My Amazing Body. Before we go, did you guess the mystery body part? The part of your body that harbours lots of bacteria is your navel or belly button! Congratulations if you figured it out.
Thank you to Dr Ming Ho and the team at Central Queensland Hospital and Health Service for telling us all about the bowel and bowel surgeries, and thanks to Kate, for sharing what it's like to live with Crohn's disease. My Amazing Body is brought to you by Queensland Health. Many thanks to my colleagues: Lauren and Jess our producers, Carol our sound technician and Helen on music and sound effects.