Hepatitis E
Queensland Health Guidelines for Public Health Units
Revision History
| Version | Date | Changes |
| 1.0 | February 2012 | Full revision of guidelines. |
| 2.0 | November 2023 | Full revision of guidelines. |
Infectious agent
The agent is hepatitis E virus (HEV), a non-enveloped, single strand RNA virus belonging to Hepeviridae family.
Case definitions and notification criteria
Report only confirmed cases.
Confirmed case
A confirmed case requires laboratory definitive evidence
OR
Laboratory suggestive evidence AND clinical evidence
Laboratory definitive evidence
Detection of HEV by nucleic acid testing
OR
IgG seroconversion or a significant increase in antibody level
Laboratory suggestive evidence
Detection of IgM HEV
Clinical evidence
An acute illness without other apparent cause with at least two of the following signs and symptoms:
- fever
- malaise
- abdominal discomfort
- loss of appetite
- nausea
AND
Jaundice OR dark urine OR alanine transaminase (ALT) ten times the upper limit of normal.
Community Outbreak Criterion
Two or more epidemiologically or genomically linked confirmed cases with no reported overseas travel.
Laboratory Aspects
PCR detection is more sensitive than serology in early stages of infection. HEV RNA is detectable in blood and stool approximately 2 weeks after infection, usually preceding illness onset. Typical specimens for NAT are serum, plasma, stool, and liver and other tissues. HEV RNA may be detectable for 2-3 months in blood, or 3-4 months in stool. Anti-HEV IgM and IgG antibodies appear about 2 weeks after infection, and IgM may persist up to 3-12 months or longer in up to 25% of cases. Anti-HEV IgG antibodies persist for life.(1)
PCR detection in serum or stool is preferred to antibody tests for the investigation of chronic infection in immunosuppressed persons.(2)
Notification procedure
Pathology laboratories
To notify on pathological diagnosis by usual means.
Attending Medical Practitioners/ Medical Superintendents (or delegates)
Not clinically notifiable.
Objectives of Surveillance
- To monitor the epidemiology of HEV in Queensland.
- To detect outbreaks of disease and enable prompt public health response.
Public Health Significance and Occurrence
HEV is the most common cause of acute viral hepatitis worldwide and has emerged as a significant zoonotic infectious disease of public health concern. HEV is estimated to cause 20 million infections leading to at least 3 million symptomatic cases globally.(3) Mortality rates are likely underestimated, though WHO estimates that HEV caused approximately 44,000 deaths in 2015.
HEV comprises of eight genotypes, four of which are known to cause human disease. HEV-1 and HEV-2 only infect humans. HEV-3 and HEV-4 infect a broad range of animal species with the potential for zoonotic transmission. HEV-5—8 are restricted to animal species, with only two reported human cases associated with HEV-7.(4,5)
The epidemiology and clinical presentation of human hepatitis E is dependent on geographical location and circulating HEV genotypes. Sporadic cases of HEV-1 and HEV-2 infection predominantly affect endemic low-income countries due to poor sanitation and contamination of water sources. Large hepatitis E epidemics have been reported in Asia, the Middle East, Africa, and Central America, and outbreaks have occurred in areas of conflict and humanitarian emergencies among refugees and internally displaced persons.(3)
Locally acquired HEV-3 and HEV-4 infections primarily occur in high-income countries, following consumption of infected animal meat or organs.(5,6) Although pigs, and therefore pork, are recognised as the main source of zoonotic infection in humans, evidence of HEV infection has been demonstrated in a wide variety of domestic and wild animals.(7)
In Australia, an outbreak of locally acquired hepatitis E was reported in New South Wales (NSW) in 2013 and 2014. There were 17 confirmed cases linked to eating Australian-sourced pork liver pâté at a restaurant, and seven locally acquired infections associated with eating other pork products. HEV-3 was detected in 16 of the 24 cases.(8)
Symptomatic hepatitis E is rare in Australia. Most Queensland cases are overseas acquired, with India and Pakistan being the most frequently reported source countries. In Queensland, 19 cases of hepatitis E were notified from 2018-2022.(9) Between 2018 and 2022, there have been 120 national hepatitis E case notifications.(10)
Clinical Features
The clinical features of hepatitis E (all genotypes) are indistinguishable from other types of acute viral hepatitis and can last up to six weeks(3). Hepatitis E in immunocompetent persons is most often asymptomatic or causes a self-limiting hepatitis. Between 5-30% of patients experience acute icteric hepatitis. The prodromal phase lasts up to one week and is characterised by fatigue, malaise, fever, vomiting, anorexia, and abdominal pain. The icteric phase progresses into the second week of illness and is characterised by jaundice, dark urine, and pale stool. The convalescent phase results in the resolution of icteric symptoms.(5)
Infections of HEV-1 and HEV-2 are generally associated with more severe acute hepatitis presentations than HEV-3 and HEV-4.(5)
Chronic hepatitis E, usually attributed to HEV-3 and HEV-4, is reported in individuals with underlying immunocompromising conditions such as chronic liver disease, liver transplant, HIV infection and haematological malignancies. Although the pathophysiological mechanisms are unclear, acute and chronic hepatitis E have been associated with extrahepatic sequalae including neurological, haematological and renal disorders, acute pancreatitis, myocarditis, arthritis, and thyroiditis.(11)
Hepatitis E during pregnancy has been associated with severe disease, fulminant hepatitis, and obstetric complications, particularly HEV-1 and HEV-2 infections. Mortality ranges from 10-30% in the third trimester. Maternal-foetal transmission can occur and is associated with neonatal clinical manifestations such as hypoglycaemia, hepatitis, and death.(5) Elderly males and those who are immunosuppressed or with pre-existing liver disease are at increased risk of severe infection with HEV-3.(4)
Reservoir
Humans are the natural host of HEV-1 and HEV-2. HEV-3 and HEV-4 are zoonotic diseases with domestic and wild pigs the likely main animal reservoir. HEV-5, 6 and 7 have been detected in many domestic and wild animal species including deer, dogs, cats, cows, sheep, goats, and shellfish.(2,6,7)
Mode of Transmission
HEV-1 and HEV-2 are mainly transmitted via contaminated drinking water, consumption of fruit and vegetables washed in contaminated water and poor hand hygiene.(5) Vertical transmission is well-understood and is associated with high mortality for pregnant people and infants.(5) HEV-3 and HEV-4 are primarily transmitted to humans via ingestion of raw/undercooked meat, meat products or organs derived from infected animals.(12)
Direct person-to-person transmission via the faecal-oral route is infrequent. Sexual transmission of HEV has been documented in men who have sex with men.(13) HEV can be transmitted iatrogenically through infected blood products and more rarely organ transplant.(5) Transfusion-transmitted hepatitis E has been documented in Europe (HEV-3) and Japan (HEV-3 and HEV-4). Routine or selective screening is performed in some European countries including the UK.(13)
Occupational exposure via direct contact with HEV-infected animals is a possible route of transmission. Seroprevalence rates have been found to be higher among pig veterinarians, pig farmers and abattoir workers.(6)
Incubation Period
The range is 15 to 64 days, with the mean incubation periods of various epidemics ranging between 26-42 days.(2,14)
Period of Communicability
The period of communicability is uncertain.
Viraemia is thought to commence prior to the onset of symptoms and last approximately 3 to 6 weeks. HEV has been isolated in stools up to 4 - 6 weeks after the onset of disease.(13)
Immunosuppression can be associated with prolonged viremia and viral shedding.(15) The infectious period may extend beyond 6 weeks in immunosuppressed individuals. Where the immunocompromised individual has a high-risk occupation, clearance may be required.(16) Longer term, serial detection of HEV RNA in serum or stool for 3 or 6 months (with or without detectable HEV antibodies) can suggest chronic hepatitis E.(14) Clinicians may consider convening an expert advisory group in immunocompromised cases with high-risk occupations to determine a plan for detecting the end of the infectious period.
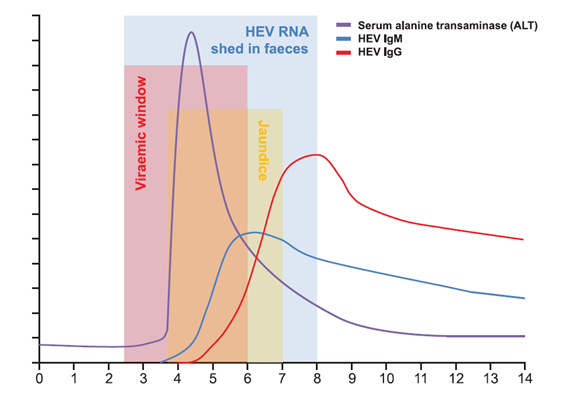
Figure 1. HEV detection in blood and stool: serological and biochemical response to acute HEV infection over time (weeks).(17)
Susceptibility and Resistance
High attack rates in young adults aged 15-49 years of age are evident in large water-borne outbreaks in low-income countries. In developed countries, the incidence of sporadic cases and seropositivity increase with age over 60 and particularly in men.(6,14)
Persons at increased risk of fulminant disease and death are pregnant people in the third trimester; persons with pre-existing liver disease; immunosuppressed individuals including transplant recipients.(2)
IgG antibodies do not provide lifelong immunity. Although the duration of protection is unknown, the likelihood of developing symptomatic hepatitis is believed to be reduced compared to non-exposed individuals.(13)
Management
Cases
Investigation
In consultation with the attending medical practitioner, determine if the source of infection is related to travel to an endemic country.
If there is no travel risk, then investigate:
- contact with a person with hepatitis E
- blood and blood product transfusion history
- consumption of undercooked shellfish and meat, meat products or organs (especially pork and game meats)
- recreational or untreated water exposure
- occupational/recreational exposure to swine, wild boar, and deer
- other potential faecal-oral exposure (childcare, sexual, social).
Determine the occupation of the case for contact tracing and restriction purposes (highest risks are for food handlers, healthcare and childcare workers).
Treatment
Treatment for acute hepatitis E is generally supportive. Hospitalisation is required for people with fulminant hepatitis and should also be considered for symptomatic pregnant people.
Restriction
Exclude from work or school during infectious period. Immunocompromised individuals may require extended exclusion based on a risk assessment considering:
- occupation
- accommodation suitability, e.g. separate toilet
- hygiene competence, e.g. hand washing skills, willingness to undertake environmental cleaning.(2,16)
Counselling
The case or relevant care giver should be advised of the nature of the infection, mode of transmission and length of infectious period (consider if immunocompromise may lengthen infectious period).
Cases should be advised, for the duration of the infectious period:
- not to donate blood(18,19)
- not to prepare or handle food to be consumed by other people
- not to share drug paraphernalia
- limit close contact with others, especially pregnant and immunocompromised individuals, and those with chronic liver disease
- to use separate toilet from household contacts, if practicable
- to practice good personal hygiene, especially hand washing and environmental cleaning (see Preventative Measures for more details).
Provide a fact sheet to the case.
Contacts
Contact Tracing
Yes
Definition
- Household contacts, or those for whom the case has prepared food or drink while infectious.
- Travel companions or others exposed to the same risk as the case.
Investigation
Search for missed cases and maintain surveillance of contacts in the case's household or persons exposed to the same risk.
Prophylaxis
Nil
Counselling
All contacts should be advised of the nature of the infection and mode of transmission. Encourage early presentation to a health service if symptoms develop, for testing for HEV. Provide advice on good personal hygiene practices, especially hand washing and environmental cleaning (see Preventative Measures for more details). Provide a fact sheet to the contact.
Preventive Measures
- Educate cases and close contacts about good personal hygiene practices, in particular hand washing and environmental cleaning:
- Wash hands with soap and water for 20 seconds and dry with a clean towel or air dry, or use alcohol-based hand sanitiser (at least 60%) if water is not available:
- before preparing and eating food
- after using the toilet or changing nappies
- after caring for someone with diarrhoea and/or vomiting.(20)
- Clean and disinfect environmental surfaces frequently and thoroughly, especially the toilet and wash basin, after use by case:
- Clean contaminated surfaces with a household detergent and water.
- Disinfect contaminated surfaces with a bleach-based household cleaner after cleaning.
- Two-in-one products reduce cleaning time (detergent and disinfectant).(21)
- Wash hands with soap and water for 20 seconds and dry with a clean towel or air dry, or use alcohol-based hand sanitiser (at least 60%) if water is not available:
- Pork, products containing pork, and game should be cooked thoroughly. A limited number of studies demonstrate inactivation by heating to at least 71 degrees Celsius for 20 mins.(22)
- Travellers to developing countries are advised to AVOID:
- consuming water or ice of unknown purity; drinking water can be rendered safe by boiling and chlorination (22)
- eating raw/undercooked foods e.g., shellfish, pork, game meat,
- eating uncooked vegetables and fruits that are not peeled or prepared by the traveller.
- At-risk individuals, such as pregnant and immunosuppressed individuals and those with pre-existing liver disease, should avoid raw/undercooked shellfish and meat, meat products or organs.
- The recombinant hepatitis E vaccine (Hecolin) is not available for use in Australia. The vaccine is licenced for use in other countries and is recommended by WHO for international humanitarian outbreak responses.(23)
- Personal protective equipment may prevent HEV infection in workers with occupational exposure to HEV-infected animals.
References
- Public Health Laboratory Network. Hepatitis E (Hepatitis E virus) [Internet]. Australian Government Department of Health and Aged Care; 2015 [cited 2023 Aug 3].
- Spradling PR, Heymann D. Hepatitis, Viral. In: Control of Communicable Disease Manual [Internet]. 2015 [cited 2023 Aug 3].
- World Health Organization. Hepatitis E Factsheet [Internet]. 2023 [cited 2023 Aug 3].
- Horvatits T, Schulze Zur Wiesch J, Lütgehetmann M, Lohse AW, Pischke S. The Clinical Perspective on Hepatitis E. Viruses [Internet]. 2019 Jul 5 [cited 2023 Aug 3];11(7).
- Aslan AT, Balaban HY. Hepatitis E virus: Epidemiology, diagnosis, clinical manifestations, and treatment. WORLD J Gastroenterol. 2020 Oct 7;26(37):5543–60.
- European Centre for Disease Prevention and Control. Facts about hepatitis E [Internet]. 2017 Jul [cited 2023 Aug 3].
- Ahmed R, Nasheri N. Animal reservoirs for hepatitis E virus within the Paslahepevirus genus. Vet Microbiol. 2023 Mar;278:109618.
- Yapa CM, Furlong C, Rosewell A, Ward KA, Adamson S, Shadbolt C, et al. First reported outbreak of locally acquired hepatitis E virus infection in Australia. Med J Aust. 2016 Apr 18;204(7):274.e1-274.e6.
- Queensland Health Communicable Diseases Branch. Notifiable Conditions System. 2023 [cited 2023 Aug 28]. Notifiable Conditions System (NoCS) QHEPS Page. (Intranet access only)
- Australian Government Department of Health and Aged Care. National Communicable Diseases Surveillance Dashboard [Internet]. [cited 2023 Aug 3].
- Fousekis FS, Mitselos IV, Christodoulou DK. Extrahepatic manifestations of hepatitis E virus: An overview. Clin Mol Hepatol. 2020 Jan;26(1):16–23.
- Said B, Ijaz S, Kafatos G, Booth L, Thomas HL, Walsh A, et al. Hepatitis E outbreak on cruise ship. Emerg Infect Dis. 2009 Nov;15(11):1738–44.
- Dalton HR, Kamar N, Baylis SA, Moradpour D, Wedemeyer H, Negro F. EASL Clinical Practice Guidelines on hepatitis E virus infection. J Hepatol. 2018 Jun 1;68(6):1256–71.
- Teshale E. Hepatitis E. In: CDC Yellow Book 2024 [Internet]. US Department of Health and Human Services; 2023 [cited 2023 Aug 3].
- Abravanel F, Lhomme S, Rostaing L, Kamar N, Izopet J. Protracted Fecal Shedding of HEV During Ribavirin Therapy Predicts Treatment Relapse. Clin Infect Dis. 2015 Jan 1;60(1):96–9.
- Taylor A, Ebert E, McMahon J, Britton L, Siebert D, Slinko V, et al. Locally acquired, human hepatitis E infection in Queensland. Intern Med J. 2020 May;50(5):643–4.
- Glynn W. Webb, Harry R. Dalton. Hepatitis E: an underestimated emerging threat. Ther Adv Infect Dis [Internet]. 2019 Apr 1 [cited 2023 Aug 3];6.
- Kumar N, Sarin SK. Hepatitis E- Is it a risk to transfusion safety? Asian J Transfus Sci. 2013;7(1):1–3.
- Bi H, Yang R, Wu C, Xia J. Hepatitis E virus and blood transfusion safety. Epidemiol Infect. 148:e158.
- U.S. Department of Health and Human Services. Show Me the Science - How to Wash Your Hands | Handwashing | CDC [Internet]. 2021 [cited 2023 Aug 23].
- NHMRC Infection Prevention and Control Team. Australian Guidelines for the Prevention and Control of Infection in Healthcare (2019) [Internet]. National Health and Medical Research Council; 2019.
- Cook N, van der Poel W. Survival and Elimination of Hepatitis E Virus: A Review. Food Environ Virol. 2015 May 20;7(3):189–94.
- Lynch JA, Lim JK, Asaga PEP, Wartel TA, Marti M, Yakubu B, et al. Hepatitis E vaccine—Illuminating the barriers to use. PLoS Negl Trop Dis. 2023 Jan 5;17(1):e0010969.