
A man sits on a couch belching and holding his stomach. On the arm of the couch are fast-food containers.
Everyone gets a digestive upset, with diarrhoea, nausea, gas, or pain, at some stage.
But if it’s ongoing, or has other symptoms, such as sores, or inflamed eyes or joints, you could have a more serious digestive condition such as coeliac disease or Crohn’s disease.
They share some symptoms, but they are different conditions. Some people can have both. So, what's the difference?
Coeliac disease
Gluten is a naturally occurring protein in—in many grains, such as wheat, barley, oats, and rye.
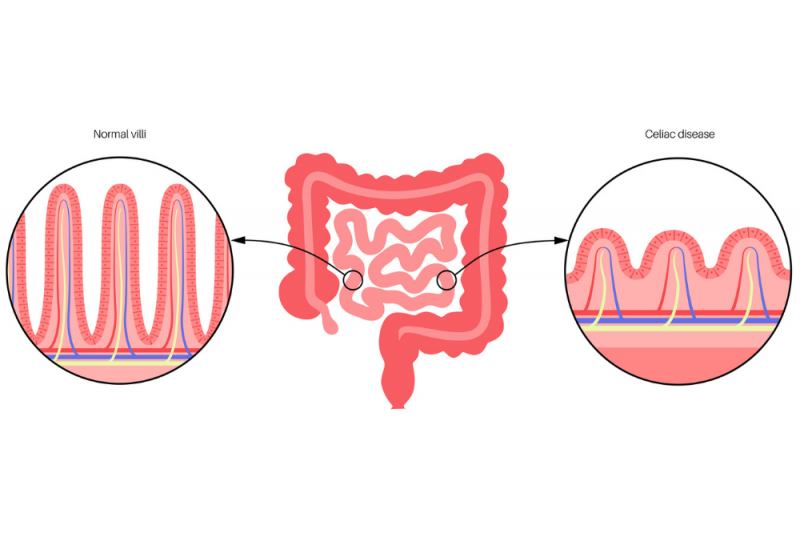
People with coeliac disease do not tolerate gluten. When they eat it, their immune system reacts and damages the lining of their small intestine. This means coeliac disease is also considered an autoimmune condition, which is when the immune system attacks part of its own body.
The small intestine has little finger-like projections called villi that help absorb food by increasing its surface area. Coeliac disease inflames and flattens them, and the damage can lead to:
- poor absorption of nutrients
- iron deficiency anaemia and/or other vitamin and mineral deficiencies
- osteoporosis
- weight loss
- gastrointestinal symptoms such as diarrhoea, nausea, bloating.
Other complications of untreated coeliac disease can include:
- infertility
- gastrointestinal cancer
- altered mental state
- increased risk of other autoimmune conditions.
Coeliac disease affects all ages, but more often (about 60%) of people who are biologically female, than male.
Crohn’s disease
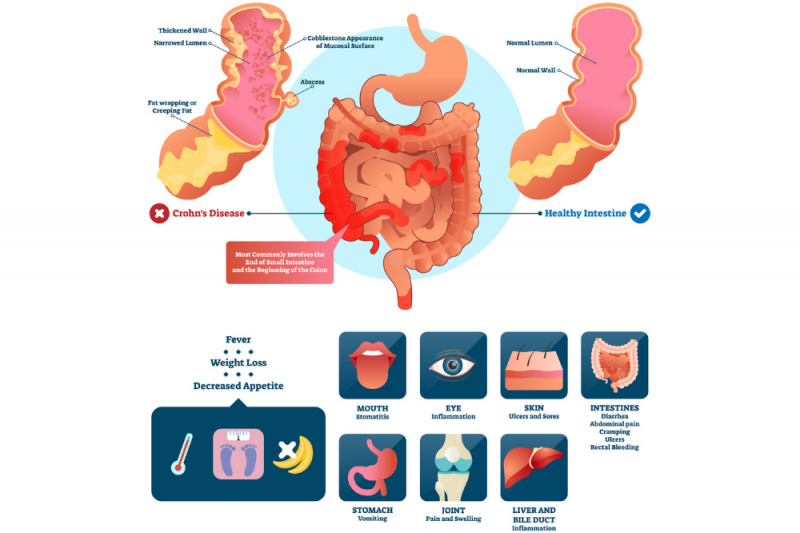
Crohn’s disease is an inflammatory bowel disease (IBD) and an autoimmune condition. It causes inflammation with swelling, tenderness, and redness in the lining of the digestive tract.
It can affect any part of the digestive tract from the mouth to the anus. But more often, the end of the small intestine and/or the large intestine.
The full thickness of the bowel can be impacted, causing narrowing, blockages, holes, and abscesses.
As the disease progresses, the following symptoms:
- the feeling of needing to pass a bowel motion more frequently, or as if they aren’t empty after
- ulcers anywhere from the mouth to anus.
- anal fissures
- fistulas (an abnormal hole between different body parts, such as intestine and another organ or intestine and skin). The most common kind is a perianal fistula (a hole near your anus)
- inflammation of joints, eyes, and skin
- shortness of breath and difficulty exercising due to anaemia
- malnutrition
- colon cancer.
Crohn’s disease happens in biological males and females equally. It can start at any age, but most commonly affects people in their late teens and 20s.
Crohn’s is lifelong and at times people can experience no symptoms, or ‘flare ups,’ which is when symptoms increase. It can be painful and impact the quality of life.
Causes
The exact causes are of coeliac disease and Crohn’s disease are unknown. Recent research suggests that the two diseases are genetically similar with a small number of genes that can make you more likely to get them. The diseases are thought to start from an interaction of certain genes with the environment, or certain triggers.
People who have one or both parents with Crohn’s or ulcerative colitis are more likely to develop it.
It’s possible that the diseases are triggered by a virus or bacterium, but scientists have not yet identified such a trigger.
Symptoms
Coeliac and Crohn’s can have these symptoms in common:
- diarrhoea
- stomach pain
- stomach cramps
- indigestion
- fever
- weight loss
- sores in mouth (cankers)
- joint pain
- anaemia
- fatigue and exercise intolerance
- rashes
- malnutrition
- slow growth in childhood (from chronic mild malnutrition)
Differences
The two diseases have important differences.
- Coeliac disease is triggered by consuming gluten-containing foods, but many people with Crohn’s can eat gluten.
- Coeliac disease does not cause inflammation of the eyes but Crohn’s can.
- Coeliac disease can cause sores in your mouth (cankers), but Crohn’s can cause sores (pyoderma gangrenosum) anywhere in or on your body, most often on your legs.
Diagnosis
Your doctor or specialist gastroenterologist will:
- take a family history
- take a list of symptoms
- order blood tests
- do an endoscopy to look at your stomach and colon and take small pieces of tissue, if they think it might be coeliac disease
- do an endoscopy, a colonoscopy, a CT scan, or MRI, if they think it might be Crohn’s disease.
Treatment
Coeliac disease
The main treatment for coeliac disease is to immediately cut out all foods containing gluten. Inflammation of the gut should then improve. If the intestine is badly damaged, some people will need treatment with steroids to reduce the inflammation. Most people with coeliac disease will need to avoid gluten-containing foods for the rest of their lives. The list includes:
- all varieties of wheat (including spelt, kamut, couscous, durum, farro)
- barley
- oats
- products using malted gluten grains such as malt barley
- rye
- semolina
- triticale (a hybrid of wheat and rye).
See Queensland Health’s gluten-free diet for coeliac disease brochure (PDF) for more information.
Crohn’s disease
There is no cure for Crohn’s disease but with medication and lifestyle changes can be managed.
Surgery is sometimes done to removed badly damaged sections of bowel.
Medications given depend on how Crohn’s disease affects a given person and can change over time. They include:
- corticosteroids to control the body’s inflammatory response
- aminosalicylates (5-ASAs) to reduce gut lining inflammation
- immunosuppressants to suppress the body’s immune response
- a newer class of drugs called biologics that use specially made antibodies which selectively bind to inflammatory signalling proteins and reduce inflammation.