
An athletic senior man dressed in running wear and shoes sits on an athletics track holding his right knee in both hands. He is grimacing in pain
Each of your body’s major joints are unique and amazing. You don’t often notice their complex and elegant functioning until something goes wrong with them.
Your knees and hips bear a lot of weight and do a huge amount of work during a lifetime.
If you are 50 years old, for example, you have lived 18,250 days. Even if you weren’t super active, and walked an average of 4,000 steps a day, you would still have done nearly 73 million steps. (Minus some steps for the first years of life.)
It’s no wonder knees and hips sometimes wear out. Disease, injury, being overweight, or unhealthy living can also speed this up.
The first sign of problems is often pain, sometimes with swelling or stiffness, that won’t go away.
Let’s have a deeper look at these important joints and why they sometimes need replacing.
Quick links
- Joints
- The knees
- Knee replacement
- Knee replacement surgery
- The hips
- Hip replacement
- Types of hip replacement
- Hip replacement surgery
- When can you go home after surgery and how long will it take to recover?
- Complications from surgery
- How long do joint replacements last?
- More information
Joints
The major joints of your limbs generally have the following parts:
- bones
- ligaments (join bones to bones)
- tendons (join muscles to bones)
- cartilage (acts as a shock absorber)
- muscles (move the joint)
- joint capsule (an envelope that surrounds synovial joints. The inner layer produces synovial fluid that lubricates the joint)
- bursae (small, slippery, fluid-filled sacs between the bits of a joint that move that reduce wear and tear)
- a blood supply and nerves.
The knees
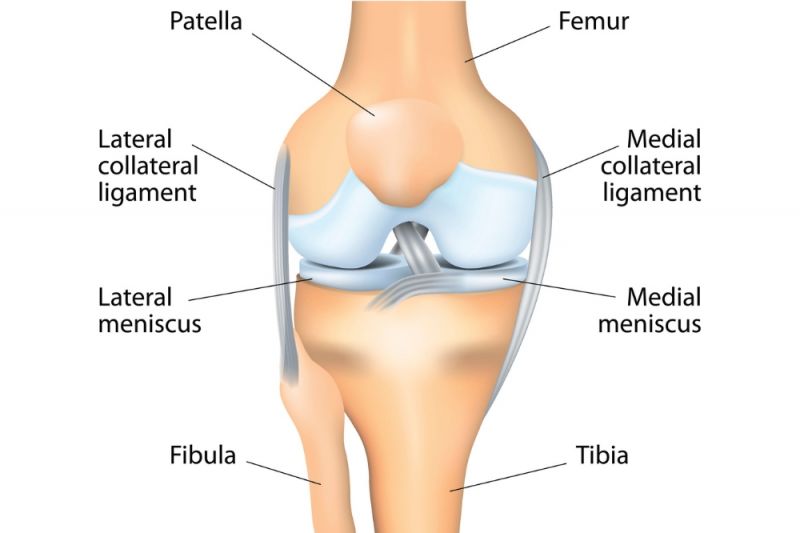
The knees are one of the largest joints in the body. They are more complex than they look. They operate like a sophisticated hinge (called a hinge-type synovial joint). They allow bending and straightening, but also some inward and outward rotation or twisting.
They join the thigh bone (femur) and the shin bone (tibia). The kneecap (patella) and the fibula (the smaller bone that runs next to the shin bone on the outside of the leg) are also connected to the knee.
Ligaments join the bones together and stabilise the joint.
Two pieces of cartilage (medial and lateral menisci) provide shock absorption between the ends of the thigh bone and shin bone.
Tendons connect the knee bones and the muscles of the leg that move the knee joint (bend, straighten, and rotate).
Knee replacement
There were 65,266 knee replacement surgeries in Australia in 2018. This is expected to grow to 161,000 by 2030.
Knee replacements are done when a person has ongoing and severe knee pain or disability. This is usually after other options have been tried, such as:
- weight loss
- low- or no-impact exercise
- physical therapy
- medications.
The most common reason for knee replacement in Australia is osteoarthritis. It’s where the cartilage at the ends of the bone breaks down due to:
- age
- overuse
- injury
- obesity
- family history
- other risk factors.
This breakdown can cause pain, swelling and joint stiffness.
Other causes of knee problems leading to replacement are:
- rheumatoid arthritis
- post-traumatic arthritis (arthritis caused by an injury)
- knee fractures
- septic arthritis (joint infection)
- bone growth disorders.
Knee replacement surgery
Knee replacements typically take one to two hours under a general anaesthetic (you’re put to sleep) or spinal anaesthetic (numbs the lower body).
In a total knee replacement, the damaged cartilage surfaces at the ends of the thigh bone and shin bone are removed. Some bone is also removed.
The removed cartilage and bone are replaced with shaped metal surfaces that are pressed into or cemented to the bone. A plastic medical spacer is inserted between the two metal surfaces. It creates a smooth and slippery surface for the metal parts to glide over. Depending on the condition of the knee, the underside of the kneecap may also be shaved back and resurfaced with a plastic button.
In a uni-compartmental (partial) knee replacement only one side of the joint is removed and replaced.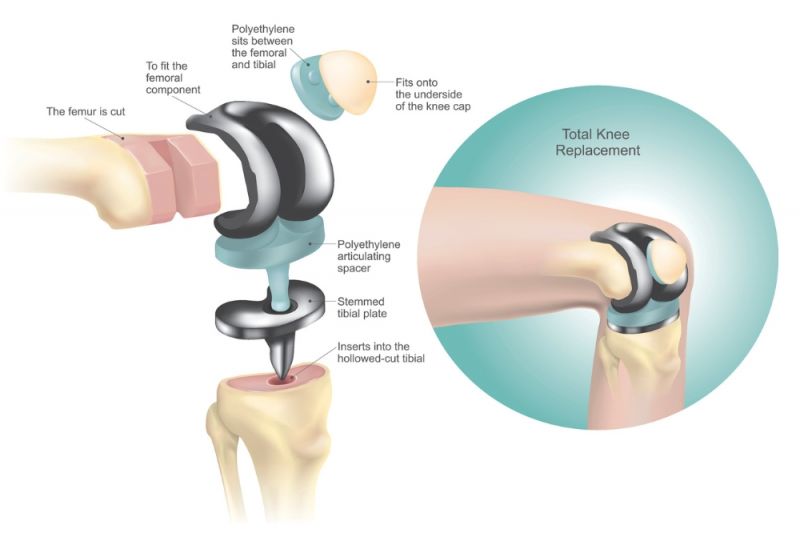
The hips
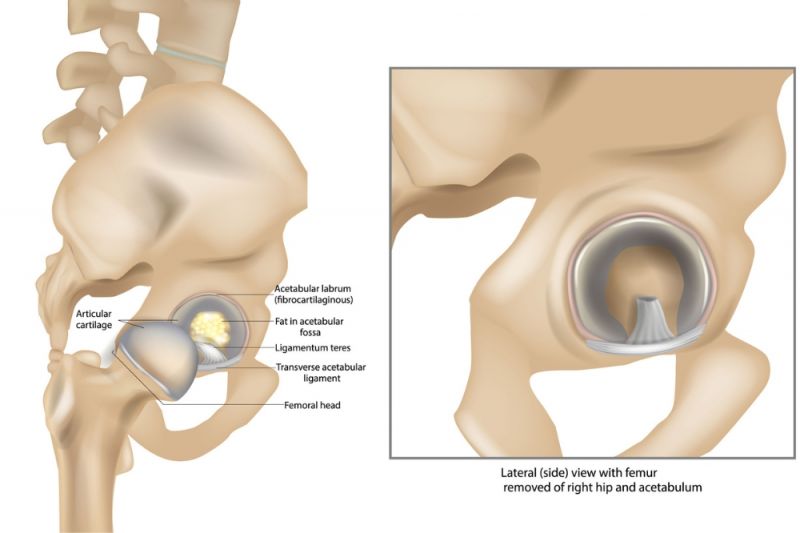
The hip joints are a ball and socket synovial joint. They join the head of the thigh bone (femur) with a depression or ‘cup’ (acetabulum) in the pelvis. There is a collar of fibrous cartilage (acetabular labrum) around the rim of this cup that makes it deeper and more secure. The head of the femur (the ‘ball’) and the surface inside of the cup are covered in cartilage.
The hip joint carries a lot of weight, so it needs to be strong and stable. That’s why it doesn’t have quite the same range of movement as other joints, such as the shoulder.
Ligaments join the thighbone to the pelvis, some inside the joint and some outside the joint. These ligaments stabilise the joint and determine how far it can move and rotate.
Many muscles are involved in the movement of the hip, knee, and leg.
Hip replacement
There were 49,764 hip replacement surgeries in Australia in 2018. This is expected to grow to 79,000 by 2030.
Hip replacement is usually done when the hip joint is worn or damaged enough that a person is in pain even when resting, and other treatments no longer provide relief. Sleep is often disturbed by the pain.
Worn or damaged hip bones and cartilage are removed and replaced with a man-made implant (an artificial hip) commonly made of metal and plastic.
The most common reason for hip replacement surgery in Australia is osteoarthritis. (See knee replacement above.)
Other reasons for hip replacement are the same as those listed under knee replacement above.

Types of hip replacement
A partial hip replacement replaces the ball at the end of the thigh bone with a metal or ceramic ball. (Sometimes just the surface of the ball is replaced, not the whole ball).
A total hip replacement replaces the ball as above, but also replaces the socket of the hip joint.
Hip replacement surgery
Hip replacement usually takes one to two hours under a general anaesthetic (you’re put to sleep) or spinal anaesthetic (numbs the lower body).
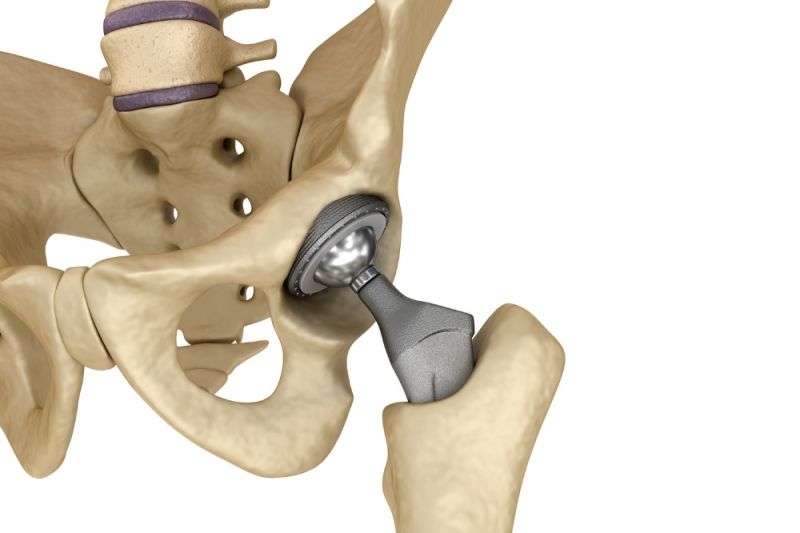
In a total hip replacement, the damaged surfaces inside the socket are cleaned out and shaped using a special tool. A cup is fitted into the socket. It can be plastic (high-density polyethylene) and cemented in place. Or it can be metal with a rough back surface so that the bone can grow onto it and hold it in place. If a metal cup is used, a plastic cup is fitted into the metal cup. The plastic is smooth and slippery and helps the ball slide around easily once in place.
The damaged ball of the thigh bone is removed. A metal (or ceramic) ball with a long metal spur is inserted into the top of the thigh bone.
The ball is then fitted into the socket, putting the hip joint back together.
When can you go home after surgery and how long will it take to recover?
You can usually go home when:
- Your pain is under control.
- Your doctors are happy with your progress.
- You can move about safely.
- You have the information, support, and care you need to manage at home.
This can be 3 to 5 days after surgery, or even sooner in some cases.
Before you leave, you’ll be given information on how to take care of your knee or hip at home. A physiotherapist will give you exercises to help strengthen the supporting muscles of the joint. You will need crutches or a walking frame to start getting around.
People recover at different rates, but you should be able to return to light activity or desk work within six weeks.
Complications from surgery
Hip and knee replacement surgeries are considered effective and safe. But all surgeries have some risks and can have complications. These risks and complications include:
- bleeding
- infection
- blood clots
- bone, ligament, tendon, nerve, or blood vessel injury
- fractures of the bone around the replacement
- dislocation of the joint
- continued pain, swelling or stiffness
- reaction to anaesthetic, equipment, or medication
- scarring of the skin.
With hip and knee surgeries, loosening or dislocation can sometimes occur in the first few months after surgery. You’ll be given exercises and physiotherapy that can strengthen the muscles and ligaments and help prevent this. You should avoid sitting on low chairs or objects, jumping, hopping, squatting, or running for at least 12 weeks after surgery. It can take up to a year to feel the full benefits of joint replacement surgery.
How long do joint replacements last?
For 90 per cent of people who have hip or knee replacements, they last at least 10 years. All joint replacements eventually need replacement (called correction or revision surgery). The younger you are when you have joint replacement surgery, the more likely you are to need revision surgery.
Research published in the medical journal The Lancet in 2017 found that only 4.4% of 60,000 people who had a hip replacement required revision surgery in the first 10 years. At 20 years, the figure was 15%.
With knee surgery the figures were 3.9% and 10.3%.
Age and sex mattered. The research found about 5% of those over 70 who had hip or knee replacement needed revision surgery.
The risk of needing revision surgery was much greater in younger people, especially men. Nearly 35% of men in their early 50s needed revision surgery.
You can maintain or extend the life of your joint replacement by:
- staying a healthy weight
- keeping up with the exercises recommended by your doctor or physiotherapist.