
What can you do to keep your arteries and veins healthy?
My Amazing Body is a podcast where we explore interesting, unknown and misunderstood parts of your body with help from medical experts and stories from real Queenslanders.
This episode is all about the arteries and veins. Cardiologist Dr Dale Murdoch explains the importance of the arteries that lead to your heart, and what happens if they get blocked. Vascular and endovascular surgeon Dr Juanita Muller talks about how your veins work (spoiler: it’s not your heart that pumps blood through your veins!) and the conditions that can affect the veins, including deep venous thrombosis, varicose veins and spider veins. Queensland woman Shelley talks about what it was like to have a DVT and then pulmonary embolism.
Meet our guests


Episode materials
Audio is great, but some things are best seen as well as heard, or might tempt you to do further reading. These materials provide more information about topics we touch on in the show.
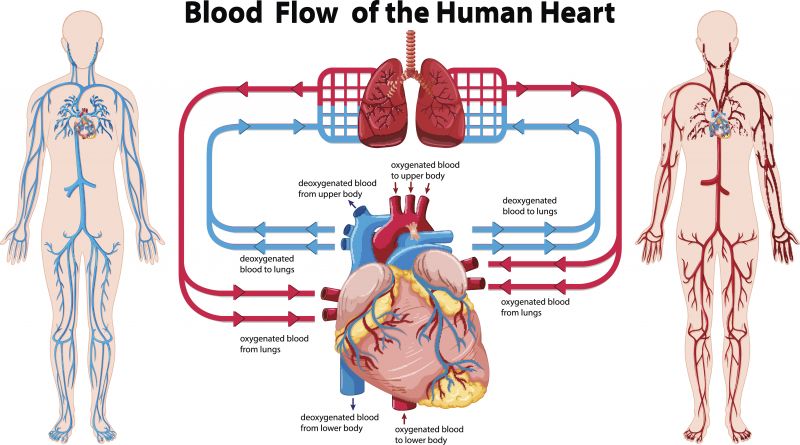
The circulatory system
Coronary artery disease and keeping your arteries healthy
In this episode, Dr Murdoch talks about how to keep your heart and arteries healthy. You can find more tips for heart health at the links below.
Health Direct: 5 ways to reduce your risk of heart disease
Heart and cardiovascular conditions
Queensland Government: Heart health
Deep venous thrombosis or DVT
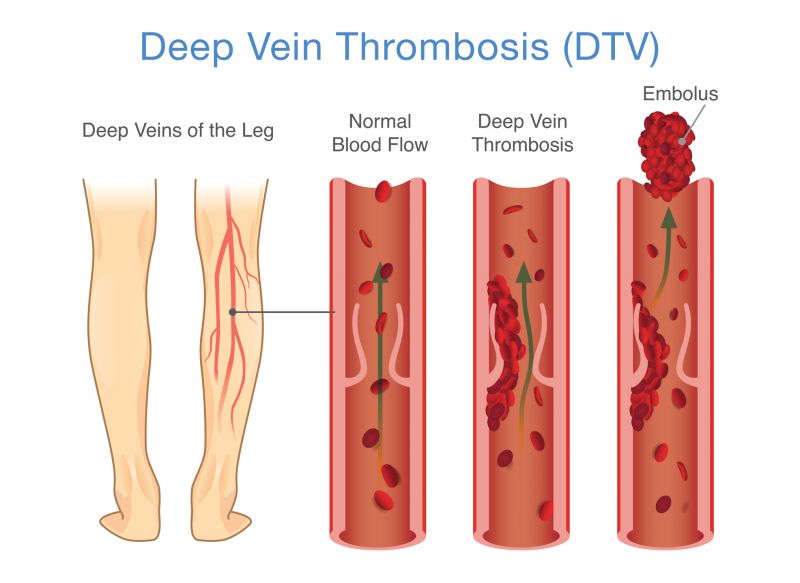
Deep vein thrombosis, or DVT, is a serious medical condition where a blood clot forms in the deep veins, usually in the calf or thigh. Not everyone with a DVT will experience symptoms, but common symptoms can include:
- pain
- swelling
- red and warm skin
- tenderness.
You can find more information about DVT here.
Varicose veins and spider veins
In this episode, Dr Muller explains the difference between varicose veins and spider veins. Below are two images which show the raised and bulging veins of varicose veins, while spider veins are flatter and smaller.


Transcript
Host: Right now, you have about 5 litres of blood moving around your body - you'll have a bit less if you're a child, and more if you're pregnant.
Your blood brings oxygen and nutrients to all the different parts of your body; it transports carbon dioxide and other waste products to your lungs, kidneys and digestive system for removal; it moves chemicals like hormones around your body; and it helps to fight off infections. It's fair to say your blood is busy, always on the move. So, how does it get where it's going?
Welcome to the latest episode of My Amazing Body, where we explore interesting, unknown and misunderstood parts of your body. Today, we're learning all about your arteries and veins.
Blood moves around your body through blood vessels. You have three different types of blood vessels: arteries, veins and capillaries. Your arteries are responsible for moving oxygenated blood away from your heart. Your veins then move blood back towards your heart - if you look at the back of your hand, you might actually be able to see some of your veins standing out under your skin - they probably look blueish in colour. The third type of blood vessel is the capillary. Capillaries spread out from your arteries to take blood to all the cells of your body. Your capillaries are tiny, with some so small that red blood cells travel through them single file.
We spoke to two blood vessel specialists, Dr Dale Murdoch and Dr Juanita Muller, about your blood vessels and how they work. First up, Dr Murdoch spoke to us about the coronary arteries.
Dr Murdoch: Hi, I'm Dr. Dale Murdoch. I'm a cardiologist here at Prince Charles Hospital in Chermside.
Yeah, so the coronary arteries are the blood supply for the heart. You might think that the heart's full of blood and it doesn't need a blood supply, but that's not true. It doesn't really get much oxygen at all from the pumping chamber, and so it requires its own blood supply. So, the coronary arteries are these three main arteries that come off the aorta, the main blood pipe that carries blood to the body, and then they move to the heart muscle and they supply the blood to the heart muscle.
So, they originate from the aorta and then they branch into smaller and smaller tubes, that go all the way down right into the heart muscle, that's a ball-shaped muscle about the size of your fist.
Host: All the muscles in your body need oxygen to work, and your heart is no exception. Oxygen is delivered to your muscles through your blood. Dr Murdoch says that if there's a blockage preventing fresh, oxygenated blood from reaching your heart muscle, you can become very unwell, very quickly.
Dr Murdoch: So, the main problem that we deal with, as cardiologists, is coronary artery disease, which is blockages or narrowing of the heart arteries themselves. So, because the heart needs its own blood supply, it's got these two to four millimetre arteries that run around the outside of the heart and supply blood. But over time they can be blocked or narrowed, and sometimes they block off very suddenly, and that's what a heart attack is.
Host: You might think of heart problems as something only older people need to worry about, but Dr Murdoch says that the causes of narrow or blocked arteries can actually start when you're young.
Dr Murdoch: Yeah, so the disease process behind coronary artery disease is called atherosclerosis, and it's cholesterol deposits that, in fact, start forming really early in our lives, often in our teenage years. And it slowly progresses over time for most people. So, if you're unlucky or you've got risk factors for heart disease, then these cholesterol plaques grow larger and larger within the wall of the heart artery. Eventually they start to cause the arteries to narrow and even block off completely.
Host: Cholesterol is a waxy substance found in your blood. About 75% of the cholesterol in your body is made in your liver, and the rest comes from the food and drinks you consume.
Dr Murdoch: So, cholesterol is when it's high in the bloodstream or when the wall of the artery's inflamed, that gets taken up into the wall of the heart artery and causes these cholesterol plaques.
Host: So, how do people know that their coronary arteries are being narrowed or blocked by cholesterol? Dr Murdoch says that it's not until they have worrying symptoms like chest pains that most people even realise there's a problem.
Dr Murdoch: Yeah, so people typically present in one of two ways. A lot of people come as an outpatient complaining of chest pain to their family doctor or to our emergency department. Most of the time that pain comes on with exertion, with stress, it might be when they're walking up a hill or walking upstairs, and they have a classic tight or heavy pain in the centre of the chest that might radiate to the neck or the arm or the jaw. Then they rest and that pain gets better.
Host: But Dr Murdoch says that just because chest pain goes away, doesn't mean there's not serious a problem.
Dr Murdoch: That tells us that there's likely a significant narrowing in one of their heart arteries. It's often not blocked completely, but it might be an 80% or 90% narrowing in one of their main heart arteries. Those patients are stable, they usually haven't yet had a heart attack, and the pumping function of their heart's often completely normal. But what we do when we see those patients, is we like to do a test to try and work out whether there is a blocked artery there.
Host: A heart attack happens when the blood supply from your arteries to your heart is completely blocked off. There are actually a few different ways this can happen.
Dr Murdoch: The other way that people present with coronary artery disease is with a heart attack. That's when there might be a moderate or sometimes severe cholesterol plaque narrowing in one of the heart arteries, and then that cholesterol plaque ruptures open and becomes exposed to the bloodstream. Then that blocks off the artery completely and often very suddenly. So those patients often have severe chest pain, shortness of breath, they're often sweaty and very unwell. When they come to the hospital, that's a medical emergency.
So, we treat those patients very rapidly. They have an ECG, they have some blood thinners. If the evidence is that the artery's completely blocked, we do an emergency angiogram, where we directly go to the cardiac catheter lab and we'd have a look at their heart arteries. If we find that one of the arteries is completely blocked, then we'd go on and do an emergency balloon and stenting procedure, and that's life-saving.
So, heart attack can happen at any age, and often young people ignore the symptoms of their heart disease. So, it is rare, but people as young as 30 or 40 sometimes do come in with a heart attack. There's a variety of reasons why people might have a heart attack when they're younger. Sometimes it's because they have a very strong family history or a type of very high cholesterol that runs in the family, and then there are some more rare causes. Some people can have a tear in the heart artery, rather than a cholesterol plaque that causes the artery to narrow or block off. That's a rare but important cause of heart attack in young people.
Host: So, what can you to keep your arteries in tip top shape and possibly prevent blockages? Dr Murdoch says that it's all about making changes to your physical activity and diet that you can stick to long-term.
Dr Murdoch: Exercise is vital for all of us in promoting heart health and avoiding heart attack. The Heart Foundation recommends that any exercise is better than none and more is better. The thing I always tell my patients is that they should find some exercise that they like doing and do that regularly. So, 30 to 45 minutes most days of the week, enough to work up a bit of a sweat and get your heart rate up. But you really have to find something that you like doing, otherwise you're not going to do it.
I think a fad gym program or something that you sign up for is a good kick along, but you really want to maintain that physical activity and exercise in the long-term. We find that people, even when they do have heart disease, that people who are active and they exercise, they have much better outcomes. They live longer and they feel better, if they exercise.
Diet changes are important also. The Heart Foundation strongly promotes a healthy heart diet, that includes a diet that's high in fruits and vegetables and whole grains. Looking for healthy sources of protein and good fats, like omega three and omega six, that are found in fish and nuts and legumes, and avoiding high amounts of saturated animal and dairy fats, is the main message regarding a healthy diet for a healthy heart.
Host: Are you ready for this episode's mystery body part? See if you can guess the body part from the clues given.
You've got two of me. On the inside, I'm lined with hairs. I have grooves filled with pheromones, which might help you to attract a mate. Another name for me is external nares.
Do you know what I am?
While your arteries are responsible for moving freshly oxygenated blood around your body, your veins bring that blood back up towards the heart and lungs. Unlike your arteries, the movement of your blood through your veins isn't pumped by your heart. Vascular and endovascular surgeon Dr Muller explains.
Dr Muller: Hi, my name is Dr. Juanita Muller, I'm a vascular and endovascular surgeon at the Princess Alexandra Hospital in Brisbane.
So, the way that our blood, as we stand, if we were to stand still, our blood just pools in a column of blood. So, if it like a big straw from your feet up to your belly, and without us walking and using our pump muscles, the blood actually has trouble getting back to the heart. And so, it's actually quite a... Because we don't have muscular pumps in the veins themselves, we've actually got to do that, and so walking's really important.
Host: Even though you can see some of your veins just under your skin, there's a lot more to the venous system than meets the eye. Dr Muller says that you have two main sets of veins - your deep veins and your superficial, or surface, veins.
Dr Muller: So, veins are really important, and they come from every part of the body back to the heart. So everywhere where there's an artery, there's also a vein. If we just talk about the legs, because that's sort of where we know most of our veins, you might see them on your skin, there's two main systems of your veins. There's a deep system, which is the really important system. So, they're the ones that actually take the bulk of the blood back up to the heart every time you move your calf. Whereas the superficial system, is kind of an extra system really, and it's just underneath the skin.
Host: Unlike the thick-walled arteries, your vein walls are thin and stretchy. This means that they can actually stretch out to accommodate more blood if necessary.
Dr Muller: You can almost see through a vein when you're operating, and you can see the blood flow underneath the surface, and so it's so thin walled, but it's really stretchy, and so it can actually get quite bigger if you're pumping more blood around.
One of those times when it gets bigger, would be pregnancy. You pump a lot more blood around your body during pregnancy, and for that reason when you look at your veins, say on your arms, just your normal arm veins, they'll be more prominent when you're pregnant than when you're not.
So, once you've had your baby and given the body a little bit of time to recover, all of that goes back down to your normal level. It's the same if you're dehydrated. So, if you've not drunk very much, your veins won't be very visible, whereas if you do drink a lot and keep well hydrated, your veins will be fuller.
Host: You've got a lot of blood vessels. In fact, it's estimated that the blood vessels of an adult could wrap around the world four times! But all it takes is a problem in just one of your arteries or veins to make you very sick.
Queensland woman Shelley found this out when at age 48, she developed a deep vein thrombosis. Shelley had recently had knee surgery and was recovering well. It wasn't until a routine physio appointment that she realised anything was wrong.
Host: While Shelley didn't yet realise the seriousness of her condition, her physio knew it was potentially an emergency situation.
Shelley: In the space of probably a couple of minutes, he went from, "Stop being a wimp," to, "I think you have deep vein thrombosis. You're very fit post-surgery, but I think we need to investigate it." He actually wanted to put me into an ambulance and send me to hospital there and then.
I rang the hospital that I had the surgery in, and they said, "Come straight away." Probably within less than an hour of my physio saying, "I think you've got a DVT," I had been readmitted to the hospital I had knee surgery in.
Host: A deep vein thrombosis or DVT is a potentially life-threatening condition. Dr Muller explains how DVTs develop and why they're so serious.
Dr Muller: A DVT stands for Deep Venous Thrombosis, and so what that really is, is clot in our deep system of our veins. So, I was talking about having a deep system and a superficial system, it's the deep system that's important. And if you get a clot in that, that's then stopping the blood getting back to the heart, so that's not good for our circulation. But the way that you will feel it, is that it causes pain, it causes leg swelling because the blood can't get back to the heart. Sometimes the leg can be red associated with the swelling, and sometimes it's even just difficulty walking. So, a bit of a limp or pain when you're walking.
So most commonly a cause by immobility, and that can for many reasons. So, it might be a long-haul plane flight, which people talk about, and we worry about when they hop on a plane, and even a long drive if you're not stopping. But then commonly it's after surgery, because sometimes you are immobile, or put into a large plaster cast, or a brace that's limiting your mobility. And like I was talking about before, you need your calf to pump the blood back up to the heart, in order to keep the blood flowing. And so, anything that stops the blood flowing, increases the ability that it might stop and cause a clot.
Host: But it's not just sitting still that can cause a DVT. Other facts can raise your risk of developing a clot.
Dr Muller: So, the other reason people get clots is because of stickiness of the blood vessels. So that can be from smoking, which does increase your stickiness, or the thickness of the blood. You can also have a family history, or other people in the family that have a clotting abnormality of some sort, and there's many, many different types of that. Again, the majority of them are quite rare, but if it does run in your family, then you are at increased risk of having stickiness of the blood.
Other things that are thought to be, is estrogen. So not so much just being a woman, but perhaps being on the pill, or a change in the pill. So, if you've been on the pill for a long period of time and haven't changed anything, your risk is probably not much higher than a normal population. But certainly, the changing of a pill, or a new start of an estrogen pill, that does increase your risk.
The other risks are, being overweight, and that is thought to increase your risk of flow, because there's less flow being able to get back to the heart.
So, one of the other causes of making blood more likely to clot, is cancer. So, you are at a higher risk of having a DVT if you're currently being treated for cancer.
And then same with pregnancy, and that's probably a combination of a lot of things. The blood's slightly thicker, you've got increased chemicals floating around the body, plus the baby is stopping the blood flowing back up to the heart quite as well as it was before.
Host: Initially, the cause of Shelley's DVT was thought to be her recent knee surgery. She was given blood-thinning medication called Clexane to shrink the blockage in her vein, which she had to keep taking by injection for months.
Shelley: A day or two later, I was actually taught to self-inject Clexane. I ended up self-injecting for about six or seven weeks at that stage. I think it was probably weekly for the first two or three weeks and then fortnightly after that for a couple of months, I would have ultrasounds of the vein just to watch the progression of the shrinkage.
Host: After she finished her treatment, Shelley's life returned to normal for a couple of months. But then she began to develop new, worrying symptoms.
Shelley: In November, I reached a really big deadline with work. I had a couple of days off and it was warming up, so I was starting to swim, just something different at the gym. I was really proud of myself this day. I had the day off. It was my first swim that I had managed to put together all of the little bits, and I swum two K's without a break. I was so incredibly proud of myself. I went home, had a shower and had to walk about 100 meters around to see a friend and was going for a coffee, and up a really, really slight incline, but walking around it and I just went, I'm just not breathing well. What's going on here?
Host: A few days later, even Shelley's colleagues could notice her changed breathing.
Shelley: I had a couple of days off, and the guys at work, when I got to work, said, "My God, your breathing is appalling. What's going on?" "Oh, it's just a virus." The next day, they went, "It's not just a virus. You need to do something about it." I went looking for a doctor that I could get into. They were so concerned about me. I was looking for a doctor down in Valley, which was where I was working, that could see me there and then. I saw a doctor who diagnosed me with something like bronchitis, asthmatic bronchitis, I think he called it and gave me a puffer and some antibiotics. I went, okay, fine. I think that might have been Thursday, Friday, and I think it was the following Wednesday I was getting worse and breathing really, really badly.
Host: Shelley booked back in with her regular GP, who was alarmed by her condition.
Shelley: I finally got in to see my own GP, and she looked at me and said, "We've got a really serious problem here. I need you to get to emergency." I went, "Oh no, I'll be fine. No, no, no." She didn't actually tell me what she thought it was, write a note. I went, "I'll just go home, and I'll do this and do that, and I've got to go and do some shopping." She went, "No, you need to go to emergency now."
Host: Shelley's doctor suspected she had pulmonary embolism - another blood clot, but this time blocking the arteries in her lungs. Dr Muller explains that a pulmonary embolism or PE can occur after having a DVT.
Dr Muller: So I suppose a PE is the thing that we worry about when you have a DVT, because a small bit of the clot that was in the leg, can break off and then go straight back up to the heart, through the heart, and then to the lungs, because that's where it's getting the oxygen for it, and that's the way that it flows. The problem is, that it gets stuck towards the lung, and then that actually then means that the lung's not getting the blood supply that it's meant to have, and so then that can actually cause death to an area of the lung.
And so, what you would feel is shortness of breath, or difficulty catching your breath, really short of breath when you're walking, whereas normally you might not have any problems. It also causes chest pains, so as you take a breath in it might be painful. And your heart rate might go a bit faster, and you might feel quite unwell.
Host: When Shelley received her diagnosis of pulmonary embolism, she also learned that her hormonal contraceptive could have been a contributing factor in developing her first blood clot months earlier.
Shelley: They said, "It sounds like you could have pulmonary embolism." I went, "What?" They explained it, and I went uh-huh. They were taking my history, and we talked about the DVT and the Clexane and all of those sorts of things. What I hadn't been asked in February was they asked about contraception. I said, "Well, yeah, I was on a low dose contraceptive." They asked me when I started it and why. I said about 12 months ago to try and help manage getting older, that certain time of life. Rather than an oral, it was a direct dose. They literally asked me to remove it there and then, instantly.
Host: It took Shelley many months to recover from her PE, and she still injects Clexane before she flies, to prevent the risk of developing another DVT. A few years on, and she describes her health as excellent, and she works hard to keep it that way.
Shelley: I think probably the thing that's most important to me now is that I have to stay fit because if I get unfit, I lose my lung capacity really, really quickly. Getting fit, staying fit, being careful around people that are aerial or have the flu. Before, I probably wouldn't have thought of a flu injection. Now I have a flu injection religiously because while I can afford to get the flu, it's just going to knock me back, and I'm going to have to work harder than most people to get my health and my fitness back after the flu or cold or something like that.
Host: Often, deep vein thrombosis will be caused by a number of factors. While doctors can't be sure, Shelley's may have been caused by a combination of her surgery and the hormonal contraception she was taking. She encourages all Queenslanders to be aware of their health and the medications they take and ask questions if they have any concerns.
Shelley: I suppose finding my DVT was accidental. I think I read the surgical risks, and maybe that was also part of the reason why I was working to get back to the gym afterwards. When my DVT was just put down to post-surgical, I just accepted it. As a 48-year-old perimenopausal woman, there might have been other factors. Now I would advise any woman to ask more questions, particularly if you're using contraceptive. Ask your GP. If you're not getting the answers you want, find somebody who will give you some answers. I think that's critically important.
Host: Have you had an experience with deep vein thrombosis or pulmonary embolism? Join the conversation on our Facebook page to share your story.
DVTs are one of the most serious, but not the only, health condition that can affect your veins. While some conditions, like spider veins, are only a cosmetic concern, others like varicose veins can pose a significant health risk. Dr Muller explains what varicose veins are and when to seek medical help.
Dr Muller: So varicose veins are really common. So about 30%, maybe even up to 50% of us will have some form of varicose veins, so someone you know, or you will have varicose veins. Varicose veins are bulges of the superficial blood supply of the veins back to the heart. And so, when you look at someone's leg, they might have a bit like a cluster of grapes on the side of the leg, and they're just bulges. And so, what happens is that, we were talking about the blood coming back up to the heart, and that's moved by the muscles contracting, but there's also valves there. And so, the muscle shoots the blood up, and then the valve stops it from falling back down again, otherwise it would go up and then down again.
And so, what happens in varicose veins is, that those valves don't work, so they don't meet. And so, the valves are too flaps, which go up and down, and they stop the blood from falling down, but if they don't meet at the centre, the blood can then fall down back through there. So that then increases the pressure in the leg vein, or in that superficial leg vein, and if you increase the pressure on a vein which is really thin walled and has the ability to dilate, it's going to dilate. And so, the main trunk, the main superficial vein will dilate, and then all the little branches off it will also dilate. And so that's how you get lots of little varicose veins all over the leg.
Host: Some people don't mind their varicose veins, while others don't like the look of them and might want them removed. But it's not just about looks - Dr Muller says that there are important signs to be aware of that mean varicose veins might need medical treatment.
Dr Muller: Varicose veins are often considered cosmetic, and people don't like the look of them. And the majority of people with varicose veins, actually won't end up with a problem. Lots of people will experience pain in their leg, and that can be really variable. So, it can be anything from, if you've walked on your legs all day, or you're a teacher, or a construction worker, or a nurse whose standing for long periods of time, by the end of the day your legs will ache if you've got varicose veins, and that might be fine. Some people are quite debilitated by the pain, they can describe itchiness and burning on the varicose veins themselves, and swelling, particularly by the end of the day.
This will be relieved by elevating the legs at the end of the day. So, if you can lay on the couch and pop your legs up, then that's the quickest way to get the fluid back to the heart using gravity again, because your valves aren't working, and that will then minimize the discomfort. The other way to minimize discomfort is, compression stockings, which you can buy from the chemist, and again, that's also counteracting gravity, so that's squeezing the blood back up to the heart.
So, pain is one thing that people do find, either a bit of a discomfort or can be quite debilitating. The time when we start to worry about it becoming a medical problem, is when people get skin changes associated with it. And lots of people won't get that, but if you notice that you've got dry skin, itchiness around... predominantly around the ankle or the skin just above the ankle, that's the area that gets affected first. Then the next phase is that you can get some brown staining of the skin, and what that is, is probably the iron from our blood.
The thing we really worry about is that, over time that can then break down, because that skin's really vulnerable, it can break down into ulcers. And only probably about five percent of people who have varicose veins, actually progress on to having ulcers. But that's clearly a really significant thing that we would love to stop happening before it happens, because ulcers are actually really hard to heal. The only way we can do that is, we can treat the varicose veins, we can elevate the legs. But it actually comes down to compressive bandaging, and that's actually a lot of hard work for the patient, it's lots of nursing, it's actually really expensive. And so, it does form a large part of the healthcare budget, out of the hospital, in the hospital, and for patients. And so, if we can stop that from happening, it makes a massive difference, especially for a patient's quality of life.
Host: So, if you have varicose veins, is there anything you can do to make sure you won't need medical treatment? Dr Muller says there's a few simple steps that can relieve uncomfortable varicose vein symptoms and prevent the skin changes that lead to ulcers.
Dr Muller: So, the simple things that you can do early on is, elevating your legs, or not sitting with your legs down for long periods of time. So, if you don't do lots of walking, and you are older, then I usually suggest when you're having your lunch or your dinner, pop your legs up on the seat beside you, so that you're not sitting with your legs down. If you've got a recliner or can put your legs up on a stool while you're watching TV, reading the newspaper, put it up, because it's actually amazing how much we sit. We might sit at work, and then we come home and sit at home. Or we might live and sit at home all the time, so the less we can do that, the better. Getting up and walking around, exercise is a massive part of the treatment, so walking keeps those valves pumping well. And then, popping your legs up when you get home, because your legs will be a bit swollen.
The other thing is looking after your skin. So, moisturizing your leg is really important. Lots of people, say in Queensland, where we're humid, you may not feel you need to moisturize your legs, but actually our skin does need moisture, particularly as we get older. And that includes men. Men don't like moisturizing their legs, but they need to moisturize just as much as women do. So, the thing I suggest is, you can even use olive oil, coconut oil, something from the grocery store that's cheap. It doesn't have to be anything fancy, but you do need to look after your skin by moisturizing. And ideally do it twice a day, but at least once a day.
And then the next step is compression stockings. Now, no-one likes compression stockings, they look relatively ugly. Most of them are beige, you can get black, you can get white, and they're relative... they can feel uncomfortable when you first put them on. But the thing that I would say is that, if you persevere, what will happen is that, some of that leg swelling will go away. And so, once that swelling has gone away, and you're back down to a normal sized leg, it will actually provide relief.
Host: So, what causes varicose veins, and how can you prevent them? Dr Muller says there are some ways to lower your risk of varicose veins, but other causes are unavoidable.
Dr Muller: So, the causes of varicose veins, we don't really understand the underlying mechanism of why it happens, but it's certainly more common as we get older in women, particularly people who stand for long periods of time in their job. It's also common after pregnancy, and it's really common after pregnancy. It's not something that women often talk about, but it's certainly very common. If we are overweight, if we've had previous DVTs, these are all reasons why you might get varicose veins, and sometimes it just runs in families.
Host: In case you were wondering, spider veins - those small, close-to-the-surface veins that might appear on the legs or arms, aren't medically concerning, though some people might opt for cosmetic treatment if they don't like the look of them.
Dr Muller: So, spider veins are just really tiny veins which are underneath our skin, lots of people have them. They look like a little patch of... like a star that's gone out underneath the skin, and they're just really, really tiny skin veins. Now they're not at all dangerous. They don't necessarily... They're not necessarily linked to varicose veins, but lots of people do have both. They're certainly... We do class them as cosmetic, and so we don't treat them in the public health system, because they won't... if you leave them there, they won't change. You might get more of them, and you might not like them, but they don't actually hurt the body. And so we do tend to leave them.
Host: As the carriers of your whole body's blood supply, your blood vessels are a hugely important part of your body. So, we asked Dr Murdoch and Dr Muller - what can Queenslanders do to keep their arteries and veins healthy?
Dr Murdoch: Dr Murdoch When it comes to coronary artery disease and heart attack, prevention is certainly better than any treatment that we have. There are lots of things that we can do to maintain our heart health. There are a few simple things that people should go and see their doctor about. That's things like blood pressure, cholesterol, getting checked for diabetes. All of those things, if treated early, can delay or even prevent heart attack for a lot of Queenslanders.
Smoking is the other thing that's vitally important to address for anyone. As a cardiologist who treats heart attacks, the vast majority of my patients who have a life-threatening heart attack, it's related to smoking. Quitting smoking's the most important thing that anyone can do to keep their heart healthy.
Dr Muller: I think the number one thing that we can do for our veins, is being as fit and healthy as possible. That's a really boring message, and no-one wants to hear it, but it's actually so important. If we were just to go for a gentle walk every day, it doesn't even have to be a long walk, and if we were to eat really good food, and drink lots of water, our veins would be so much healthier. And it really then does reduce what the long-term burden of having varicose veins or having unhealthy veins.
Host: Thanks for listening to this episode of My Amazing Body. Before we go, did you guess this episode's Mystery Body Part? Your hairy, pheromone filled external nares are your nostrils! Congratulations if you figured it out.
If you found this episode of My Amazing Body interesting, please consider giving us a rating or review, to help other people find our podcast.
My Amazing Body is brought to you by Queensland Health. With special thanks to our expert guests Dr Dale Murdoch and Dr Juanita Muller, Shelley for sharing her story of having DVT and PE, the media teams Metro North and Metro South Hospital and Health Services and my podcast colleagues - Lauren our researcher, writer and producer, Carol our audio technician, Dan our music guru and Helen on sound effects.