How does your brain control your bodily functions?
My Amazing Body is a podcast where we explore interesting, unknown and misunderstood parts of your body with help from medical experts and stories from real Queenslanders.
This episode is all about the Brain, with a focus on how your brain helps you move. We spoke to neurologist Dr Alex Lehn from the Princess Alexandra Hospital about how your brain controls your bodily functions. He also explains what functional neurological disorders (FND) are and how they affect the body. Then, Queenslander Christine talks about her experience with FND.
Meet our Guests


More information
The Brain 1.0
To learn more about the different parts of the brain listen to episode 13 of season one.
Functional neurological disorder
For more information on functional neurological disorders visit FND Australia.
Transcript
Host: What are you doing right now? You might be walking, cooking, driving around or just sitting down. You're definitely breathing and, hopefully, you're listening to my voice. You're doing all of these things, and for the most part, you're not thinking about them. You're just...doing them. How is it you can do all these things, and many others you're not even aware of, automatically? And what happens if those actions suddenly become less automatic?
Welcome to this episode of My Amazing Body, a podcast where we explore interesting, unknown and misunderstood parts of your body. Today, we're learning about your brain function.
You might remember we explored the brain back in episode 13 of season one, with epileptologist Dr Sasha Dionisio. We (and a lot of you) found it so fascinating that we're revisiting the topic. But this time, we're focusing on how your brain effects the way you function in day-to-day life.
We spoke with Dr Alex Lehn from the Princess Alexandra Hospital all about how the brain enables you move around and perceive the world.
Dr Lehn: My name is Alex Lehn. I'm a neurologist here in Brisbane and I run the movement disorder unit here at PA Hospital. So really, my main job is I'm a movement disorder neurologist, so I look after people with things like Parkinson's and tremors and gait disturbances and those things. Together with my neurosurgeon, Sarah Olson, I also run the deep brain stimulation service here at PA Hospital.
So that's if you want my day job. My real passion in life, though, are functional neurological disorders, which is a group of disorders I feel very passionate about them. A group of patients I feel very passionate about.
Host: Before we delve into Dr Lehn's passion for functional neurological disorders, we wanted to know, how does the brain control your bodily functions?
Dr Lehn: So there are multiple parts of the brain that are involved in that, and that's something where we learn nowadays more and more. Like from the old days, we kind of thought, "Oh, this part of the brain is in charge of sensation and this part of the brain is in charge of motor function, and this part of the brain is in charge of memory." And while there are certainly specialized areas of the brain for certain functions, what we learn more and more is there are multiple areas that need to work together well in order to do that.
Host: As you might expect, brain function is complicated; there's a lot going on, all the time. So, let's break it down - how does movement work?
Dr Lehn: So if you think about it, the human brain, we've got two main ways to control our movements. One is conscious control and the other one is automatic control. And we can consciously control pretty much all the movements there are, but if you think about what you do in everyday life, literally everything we do is done automatically. So if you, I assume sit in front of your computer at the moment, or a listener sit in their cars or in front of their iPods, you don't have to think about how you sit, you don't have to think about how you stand, how you walk, how you talk even. All these things are done automatically. And they're really complex things to coordinate for the human brain.
Host: You're probably not thinking about it, but right now, you're making heaps of automatic movements. Some of them you'll choose to do, like moving your arm to pick something up. Others are happening automatically, like the tiny muscles that are working to keep you upright and stable if you're standing or sitting.
Dr Lehn: Ifyou think something like walking, when you need to flex this muscle, extend this muscle, shift weight on that side, all these kind of things, we don't have to think about it at all. Even something as simple as sitting upright, where your body constantly, every millisecond, needs to sense if it's upright or swaying to one side and correct for that without you even thinking about it, or talking. Like me talking at the moment, there are dozens of muscles you need coordinated in perfect harmony to get words out in an understandable way.
So while these things are hard to learn and, you know, if you think as a toddler, it takes as many years to learn to control these kind of movements, the human brain knows these are things I have to do a lot, these are things I have to be very accurate with, and these are things I want to be very energy efficient with in the future. So, once we learn those kind of pathways, they actually get kind of hardwired into the brain. And once we learn those, don't have to think about them anymore. You can trigger them off automatically.
Host: But it's not just all about muscles and movement. The way you perceive the world - the sensations you receive that tell you what's going on around you and the thoughts you have about what you want to do - influence the way you function as well.
Dr Lehn: So, as you can imagine, to coordinate the movement, you need to have sensation working as well. Like it gives your body feedback and you need some control mechanisms in the brain that not only move something up and down, but control things in a better manner so you have got some smooth movements as well. And you need cognition as well to plan those kinds of things. So, lots of different areas are really involved with that.
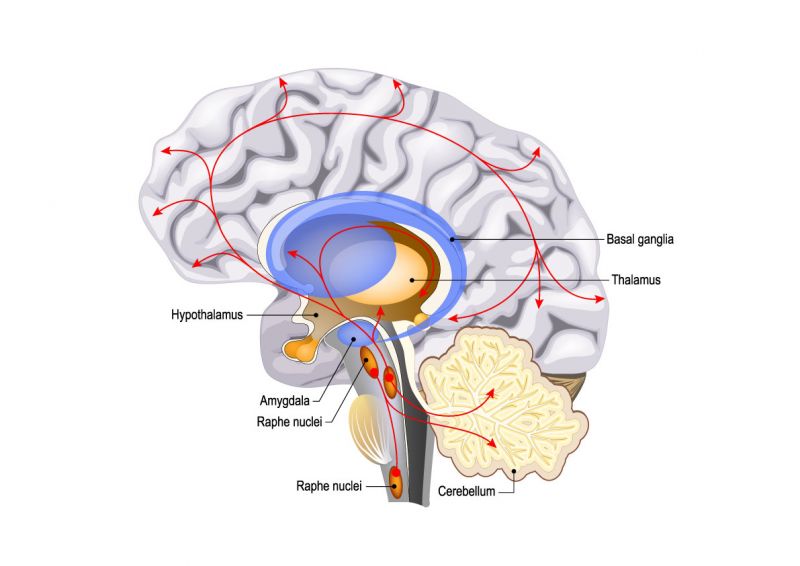
And there are motor pathways and sensory pathways, kind of the input and output mechanisms of the brain, but then in between as well, you kind of need areas of the brain that coordinate and put all those different paths together of cognition, planning, output then towards the motor pathways, and really that's done in the basal ganglia.
Host: Your basal ganglia are a network of structures deep in the base of your brain, that help the different parts of your brain send messages and communicate with each other. They're involved in everything from your movement, to your thinking and emotions. Dr Lehn says they're a really important part of your brain, and when he works with patients with neurological disorders, it's often these basal ganglia that are affected.
Dr Lehn: So, the main area that's affected in patients with Parkinson's disease are those basal ganglias, and the difficulty they have is not so much weakness or not so much problems with sensation, but really with coordination of movements. Or another example would be people with Tourette's, people might know or might have heard about, or Huntington's disease. So, all those diseases really cause difficulties and abnormalities in that basal ganglia function.
Host: Dr Lehn works with two main groups of patients: people with organic neurological disorders and people with functional neurological disorders. From the outside, both of these types of disorders might seem like they cause similar symptoms, like a difficulty controlling movement or speech. Dr Lehn explains that understanding the difference between the two types of disorders is similar to understanding what's going on when you have a problem with your computer: is it the physical parts of the computer that are damaged, or is it the software that's glitching and causing the issue?
Dr Lehn: So probably a good way to look at that is if you think of your central nervous system, so brain and spinal cord, so think of it like a computer. And in that computer, there's two ways things can go wrong. So one is you can do damage to the hardware parts of that computer, and that's kind of all those traditional or those organic diseases, like if you have a stroke, you knock out a bit of the cable work in your brain, or Parkinson's disease, as I explained beforehand. What happens in Parkinson's disease, because of neural degeneration, so unfortunately certain parts of the brain die off quicker than they should and because of that, they get damage into those parts of the cable work. And so on are brain tumours or multiple sclerosis. What they all do is they knock out certain parts of that cable work in our brain.
Host: Chances are, you've known someone with an organic neurological disease like Parkinson's or multiple sclerosis, or someone who's had a stroke, tumour or aneurysm that's affected their brain. If not, you've definitely heard of these conditions. But Dr Lehn says functional neurological disorders, while extremely common, are much less well known.
Dr Lehn: The other way we can get in trouble is software. How the software can start misfiring. And really that's what happens in functional neurological disorders, is it's a brain software disturbance. And really what we mean with brain software is actually communication. That's what goes wrong, how the brain communicates within itself. So those different parts, what we alluded to beforehand, of the brain, how they communicate with each other to function properly, that doesn't work anymore. The communication between brain and outside world can glitch and not work properly anymore. And the communication between brain and body, and vice versa, so how the brain controls certain body parts, but also how that sensory feedback from the body to the brain glitches and doesn't work properly anymore.
Host: Are you enjoying My Amazing Body? Why not leave a review or rating in your podcast app, to help others find our podcast and learn all about their bodies, too!
Are you ready for this episode's mystery body part? See if you can guess the body part from the clues given. We'll reveal the answer at the end of the episode.
I'm soft and fleshy and shaped like a tear drop.
I stop food from going places it shouldn't, like up your nose, and I also make saliva.
My name comes from the Latin word for 'little grape', because that's kind of what I look like.
Do you know what I am?
A 2019 National Health Commission report found that functional neurological disorders (or FND) are the most common diagnoses in neurological practice and are actually the second most common reason a person in Australia will go to a neurologist when they're experiencing headaches.
Dr Lehn: There's a lovely neuropsychiatrist in Melbourne called Richard Kanaan. He's one of the experts in the field of functional neurological disorders and he gave a talk not too long ago, and in that talk, he said, "This is the most common disorder people have never heard of." And it's absolutely true.
Host: FND isn't a new disorder but understanding of it is still growing among medical communities and the public.
Dr Lehn: FND has been there since human brains have been there. The human brain is a complex beast, and it's easy to misfire and easy to glitch. Since human brains have been functioning, there were glitches there and the first descriptions of really what was FND already described in 3000 BC, and if you go back in medieval times, FND has always been there.
And also, I should point out, we don't think it's actually more common nowadays than it was in the past. Some people say, "Oh, it's because nowadays people are so neurotic and hectic times and we push ourselves so much." It's probably not true.
Host: In Australia, about 50 in every 100,000 people will experience FND. So, what is this condition? Dr Lehn says it's what happens when some of those automatic processes normally controlled by your brain without you having to think about them, like walking, stop working properly.
Dr Lehn: What goes wrong, for example, in patients with functional movement disorders, to give that example, is that those patients or those people accidentally override with conscious control what should be done with automatic control it.
Host: If you've ever had trouble swallowing a medicine tablet, even though you don't have any issues normally swallowing your food, Dr Lehn says you know what it's like to experience these mild functional symptoms.
Dr Lehn: I think one very good example, for me, that my wife told me once, who is a speech pathologist, is swallowing. So, if you think swallowing, again, is automatic as it gets. So, believe it or not, we produce two litres of saliva every day, all of us. And we swallow, day and night, awake or asleep, usually all automatically all that saliva even without thinking about it. You can consciously trigger off a swallow. Just try that and swallow some saliva. Sometimes it feels a bit awkward, but we can do it. But probably a good example how those conscious controls overriding automatic controls and getting problems with that is probably swallowing tablets.
I think most of us know that feeling. If you're not a good tablet swallower, when you take a Paracetamol or a Nurofen tablet for a headache, how hard it sometimes can be to get those tablets down. When you put a tablet in the mouth and just try to get it down your throat, it feels really weird, really awkward, I have to force it down. Glass of water. It doesn't go down.
And often people say, "It's because those horse tablets are so big," but it's actually not true at all. The average tablet is much smaller than the average piece of steak that you swallow. It's really, the problem with that is us overriding with conscious control what should be just an automatic swallow.
And for most of us, as soon as a tablet is down, afterwards, we go back to whatever. Have dinner or have a piece of cake, no worries at all. We can swallow those other things. Back to normal again, and all. But what happens, for example, in those functional movement disorder patients is that they get stuck in this override with conscious control what should be automatic.
Host: For many people living with FND, the symptoms of the condition are much more severe than having trouble swallowing the occasional tablet. Dr Lehn says that because the range of functions the brain controls are so broad and complex, so are the symptoms of FND.
Dr Lehn: If you think if the brain software starts glitching and the brain is on edge with its function, it doesn't fire on all cylinders anymore, it's never going to show itself just in one symptom. So out of a few hundred patients I see a year with FND, I've never seen a patient with just one symptom. If you actually go through the history, literally for all patients with functional neurological disorders, have several symptoms. And many of them, multiple symptoms. Often patients, when we start making a list of all the symptoms, they have to come up with 5, 10, 15, 20, 25 different symptoms they actually have.
Host: FND can also affect how a person processes sensory input, their cognitive function or thinking, and their emotions.
Dr Lehn: Really, any function that's controlled by the human brain can be affected. So, as we said, since we function, for example, so really kind of funny, abnormal, over-sensitivity that comes and goes or numbness that comes and goes, all varieties of abnormal movements from functional tremors to uncontrollable shaking, to functional weakness, for example. I've got patients that either can't move certain body parts or sometimes the whole body. Can't control the whole body anymore. Can't move it at all.
Cognitive dysfunction is very common. So, people often come in with brain fog, just really difficulty with concentration. Those kinds of things. Speech, very common. So, word finding difficulties or stuttering, sometimes completely unable to speak. So really one of the hallmark features of functional neurological disorder is really combination of multiple neurological symptoms and extreme variability with these kind of symptoms.
Host: So, what causes the brain software to glitch in this way? Dr Lehn says it sounds like a simple question, but the answer, like most things related to the brain is far from simple.
Dr Lehn: So why people develop functional neurological disorders, what we use for it nowadays is what's called the biopsychosocial framework. Bit of a mouthful. I'll break it down for you. So, there are biological factors that play a role. There are psychological factors that play a role. And there are social factors that play a role. And amongst those are some that make the brain vulnerable towards developing functional symptoms. There are triggering factors that set off functional symptoms. And there's what's called perpetuating factors, or factors that prevent people from recovering from the symptoms they have.
Host: Dr Lehn says that these genetic factors, psychological factors and a patient's personal history all combine to create the opportunity for FND to develop, but that the final trigger for the brain to start glitching in those messages it sends might not seem that significant.
Dr Lehn: And the last trigger we see, the last kind of straw that breaks the camel's back, is often something relatively minor. So, you often see patients and they come in and say, "Oh, it's just kind of a bit of a cold flu, or I was a bit run down because work was really stressful lately." When you think nothing really significant, or maybe a faint in a patient or a fall otherwise. But it's often, what you see when you actually go to the history, it really seems unfortunate. All the other factors have lined up just in the wrong way, and then that last trigger that comes along is just what pushes the brain over the line into those function symptoms.
Host: We spoke with Queensland woman Christine, who lives with FND, about her experience with the disorder. She says that after living with a different chronic health condition for years, at first, she didn't twig that something was going on with her movement.
Christine: My FND symptoms first started in 2016 when I was recovering from another chronic illness. The way it presented to me was with sort of an inability of my right leg and my left arm to actually automatically move properly when I was on my walks. So, it was a slow introduction to FND in the sense that they were not major symptoms, though it was concerning that I had to keep driving this arm and this leg to actually keep in time when I was actually walking. All I knew was that I had to drive that motion, I had to push myself to actually keep that rhythm and when I actually was in that rhythm and walking quite fast it would be okay, but when I slowed down I found my mind having to keep telling my arm and leg to keep moving.
Host: Christine did talk to her doctors about the new symptom and was told perhaps it was related to the stress of her previous illness. Her GP referred her to the Princess Alexandra Hospital neurology department, where Christine got a diagnosis of FND. At first, her symptoms didn't really change, and Christine, an academic, kept living her normal, busy lifestyle. But then things got much worse.
Christine: For probably another year and a half, I was in a new academic role, which I thoroughly enjoyed and I had a lot of commitments, a lot of long-term goals that I was progressing towards. I went overseas for work several times and I just put it all on the back burner, really. I was able to actually manage my life, it wasn't still a significant part, but unfortunately, I was moving myself to exhaustion really, and I had a couple of warnings when I was overseas. My top of my shoulder, my top of my arm didn't work properly but I would just kind of push through.
At one point actually on the plane home, I had, I would say now, like a dissociative episode where even the flight attendant was saying, "Are you okay?" And I could hear them but I couldn't actually speak. I was getting little symptoms there of you need to be careful. I suppose in my mind I thought, well, all of these big commitments will be over at this date, and then I'll start to rest. But I couldn't get out of the fatigue, really, myself.
Host: Along with these physical and psychological symptoms, Christine began to experience another very worrying effect of FND.
Christine: Well, during that time I did actually have another symptom that was starting to occur, and it was a very different type of one. It was, I felt that I was going to fall downstairs. So, this related particularly to my work area when I had to walk up and down the stairs, I had this feeling I was falling, and I was getting very worried about that because I didn't want it to impact my work.
Host: By this point Dr Lehn had become Christines' treating doctor, so she's was learning more and more about FND and how it could be treated.
Christine: So that hit home a little bit more and I did actually talk to Dr. Lehn about that, and he recommended the two-pronged approach, I guess we have mainly with FND, and that's a physiotherapist that understands FND, and also a psychologist that would be able to understand that as well.
Host: But Christine's busy lifestyle didn't allow her to fully rest and recover, and in September that year she had a severe episode of FND symptoms which landed her in hospital.
Christine: So, it wasn't until in September of that year I had this very dramatic event where I was actually shopping in the supermarket and lost control of my left arm completely, it was just hanging by my side, I couldn't do anything. By the time that I got home my left leg was the same, and I couldn't speak properly. So obviously myself and my family thought I might be having a stroke, so we did actually call the paramedics.
By the time I got to the emergency department I was so photophobic I didn't even want to look at anything, I had a towel over my head just to avoid all the lights. So that was the real sudden episode that I had, completely life changing really, that brought me into the reality of what functional neurological disorder means to you.
I was in hospital for two and a half weeks. I basically had to learn how to walk again, and so it was a very levelling experience, I can say, because one minute I'm a successful academic talking to hundreds of people, doing these projects, and the next minute I'm lying in a bed and I can't even get out of the bed by myself.
Host: Dr Lehn says that treatment for people with FND focuses on switching their brain back over into automatic mode, and he often refers patients to multiple specialists to help.
Dr Lehn: The treatment often is surprisingly simple, if you want. There's actually no real rocket science to it. The idea is can we help these patients to retrain their brains? And typically, in a typical patients, that means multidisciplinary therapy with ideally therapists who have some expertise in the treatment of functional neurological disorders. And for an average patient, that would mean treatment by a psychologist and a physiotherapist, depending on what symptoms they have, with expertise in that area with what the majority of our patients undergo, to really try to... okay, can we teach and help those patients to relearn, for example, as we had the example before with functional movement disorders, to relearn normal motor pathways and normal motor function.
And the actual therapy is often... it's nothing super fancy. Often, I feel, dare I say, something a bit like a fraud when we get patients in and they expect we've got some magic apparatus or so, and at the end, it's literally just a lot of common sense, relatively basic things we teach patients. But it can be really successful and really effective.
Host: Unlike a patient recovering from a physical brain disorder, like a stroke, where it's important for them to focus on the task at hand to retrain the brain, FND patients need to try to get their brains functioning without their thinking about it. Dr Lehn says there are lots of ways to trick the brain into this kind of action.
Dr Lehn: The issue is, in functional neurological disorders, that we override with conscious control what should be done automatically. And the harder we try, then, with even more conscious control, the worse we're going to get with it, with that overriding.
So, one of those things we try to teach people, which initially sounds very counter-intuitive, is exactly that. The idea is not like we're trying to build up those muscles again, like with other diseases. Muscles are not the problem. The problem is how the brain talks to those muscle groups, for example. With those distraction techniques, for example, really what we try to achieve is can we distract your conscious attention and your conscious control away from those pathways to then re-allow automatic pathways to occur again?
And again, the principles are really simple. For many patients, what we do is we often teach them, for example, is counting backwards, for example, as a distraction. A classic one we see are sevens, because counting in sevens is a reasonably hard thing to do for the brain. So, we tell patients, "You just start 100 and you subtract 7 away from it every step, to get something else for the brain to do."
Host: During her time in hospital and afterwards, Christine had to learn to walk and talk again, as well as addressing her sensitivities to light and noise, a process that took a long time.
Christine: Basically Dr. Lehn came in that day and said, "Really all I can offer you is hard work. There's no one pill that will fix this." I felt sorry for myself for about a couple of hours, and went, "Oh no." So, then I thought, well there's no other way, I have to actually put myself to the task and actually I worked very hard for all that time. And I was very fortunate that the quick treatment and understanding actually helped me be able to walk again.
My speech came back a fair bit but I still have some trouble with that, and I had a lot of work with the physio about addressing loud noises and being able to... the bright lights, so that type of thing. So, there was a lot of results of that particular event. I think besides all the hard work you're doing in all those areas, which went on for another few months, I was off work for 70 days overall and I was very fortunate to have a daughter who's a physio who came over every day and actually ran me through the exercises and things.
Host: These days, Christine says she lives well with FND, but the condition still affects her and possibly always will.
Christine: There was these two prongs all the time. Fatigue was a very big thing and still is, that you could be physically exhausted but also mentally exhausted. So how to actually manage that, so I still have physical symptoms. If I'm tired, I find it hard to walk, I have some weakness in my arm, my speech is slurred sometimes in some very quirky ways, like trying to order a coffee at the coffee shop it will be very slurred. Then I turn to my daughter who might be with me and say, "Can you tell them what I want please?" Or I misjudge things because I'm not quite sure where I am, and I have had difficulty swallowing.
So that's one part, that's the physical kind of things that you have to manage, but I also have trouble with sensory things too, so sensitivity to noise, to lights, to a lot of movement. Emotionally I think I overreact sometimes to things that are happening, and I have actually experienced going away and dissociating myself from things as well, but probably the biggest one is the fatigue and sometimes the anxiety that comes with that, of trying to manage all of these things.
Host: If you think you or someone you know might have functional neurological disorder; Dr Lehn recommends talking to a doctor about it. He also recommends that people who are interested in FND, who have been diagnosed with FND or medical and allied healthcare professionals interested in learning more about FND should visit the fndaustralia website, we've added a link in the show notes.
Dr Lehn says he enjoys working with patients and helping them to understand their condition.
Dr Lehn: I really enjoy sitting down with a patient and talk to them, explain to them, and make them understand, to help them along the way, and make them understand. To be able to help themselves more afterwards as well, that's something I really enjoy.
And that's, as you can imagine, in the public setting, often difficult, because there's often little time to actually sit down and explain things in more detail. But that's something I find very satisfying, to do that well, and that's what I probably enjoy most, I think.
Host: Thanks for listening to this episode of My Amazing Body. Did you guess the mystery body part? The fleshy tear drop is your uvula, not your tonsils as many people believe. Congratulations if you got it right.
Thank you to Dr Alex Lehn and the team at the Metro South Health and Hospital Service for lending their time and expertise to this episode and to Christine for sharing her experience with FND.
My Amazing Body is brought to you by Queensland Health. Thanks to my podcast colleagues, producers Lauren and Jess, Carol our audio technician and Helen on music and sound effects.