
The lungs are the organs in your body that help you breathe
My Amazing Body is a podcast where we explore interesting, unknown and misunderstood parts of your body with help from medical experts and stories from real Queenslanders.
This episode is all about the lungs – one of the most important organs in your body. The Director of Respiratory and Sleep Medicine at the Princess Alexandra Hospital in Brisbane, Dr Michelle Murphy describes the different parts of the lungs, how you breathe and how your lungs work with rest of your body. Dr Michelle Murphy also explains the impact COVID-19 can have on your lungs. Then, Queenslander Josh talks us through what it’s like to have a collapsed lung.
Meet our guest
Episode materials
Audio is great, but some things are best seen as well as heard, or might tempt you to do further reading. These materials provide more information about topics we touch on in the show.
Asthma
Over 2.5million Australians live with asthma, making it the most common chronic disease affecting our population. You can find out more information below.
5 things you might not know about asthma
The below video made by Asthma Australia shows how asthma can affect a person's airways.
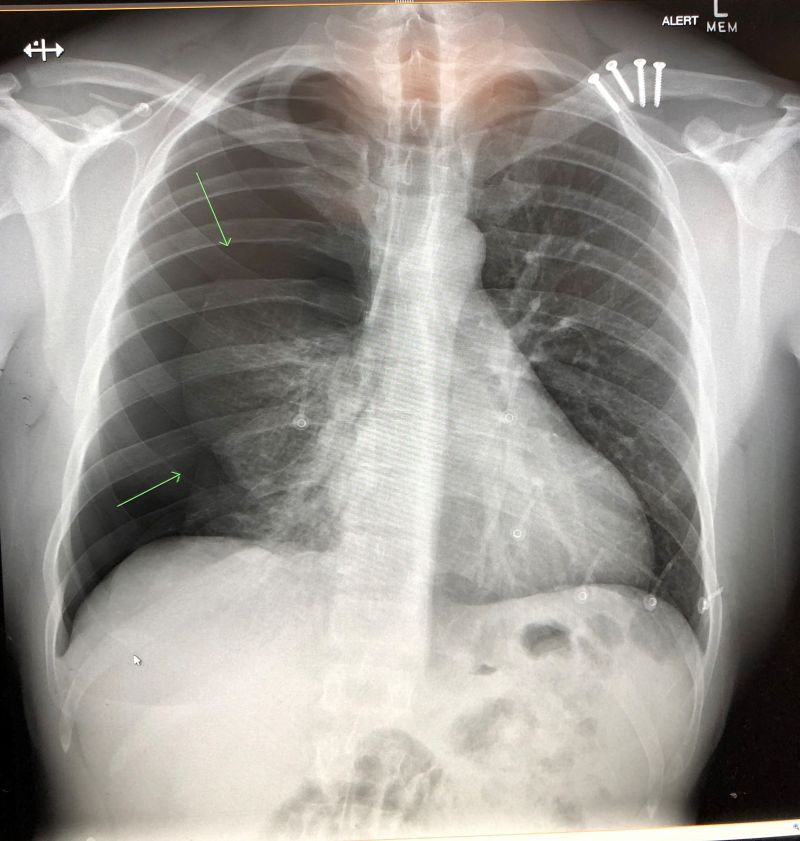
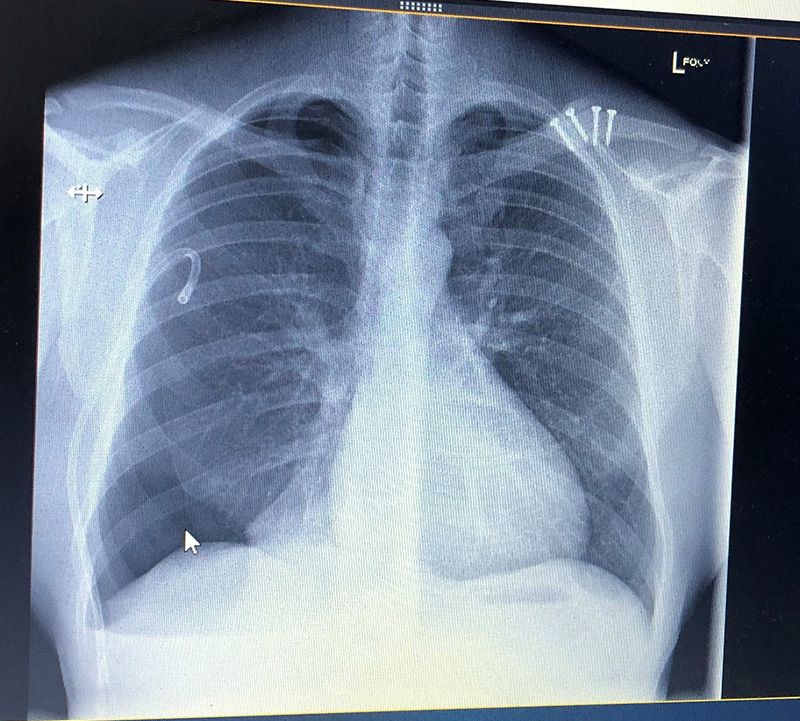
X-ray of Josh's collapsed lung
Transcript
Host: The average adult takes around 12 to 16 breaths per minute, without ever really giving it much thought. But I bet you're thinking about it now. How much do you know about what happens when you breathe? With every breath there's actually quite a lot going on.
Welcome to this episode of My Amazing Body, a podcast where we explore interesting, unknown and misunderstood parts of your body. In this episode we are learning about the lungs. What exactly do they do? How do they do it? Why are they sometimes compared to trees, and what can happen if something goes wrong with them? Keep listening while we explore these questions and a whole heap more.
Dr Murphy: The lungs are the organs in your body that help you breathe. In my opinion, they're the most important part of the body, because your entire body doesn't work if you're not able to breathe. So, what your lungs do is when you take a breath, they take that air down into the lungs and they absorb all the oxygen, that then goes to the rest of your body to help your organs work.
Host: That was Dr Michelle Murphy, the Director of Respiratory and Sleep Medicine at the Princess Alexandra Hospital in Brisbane. I think we can all agree that our lungs sound pretty important.
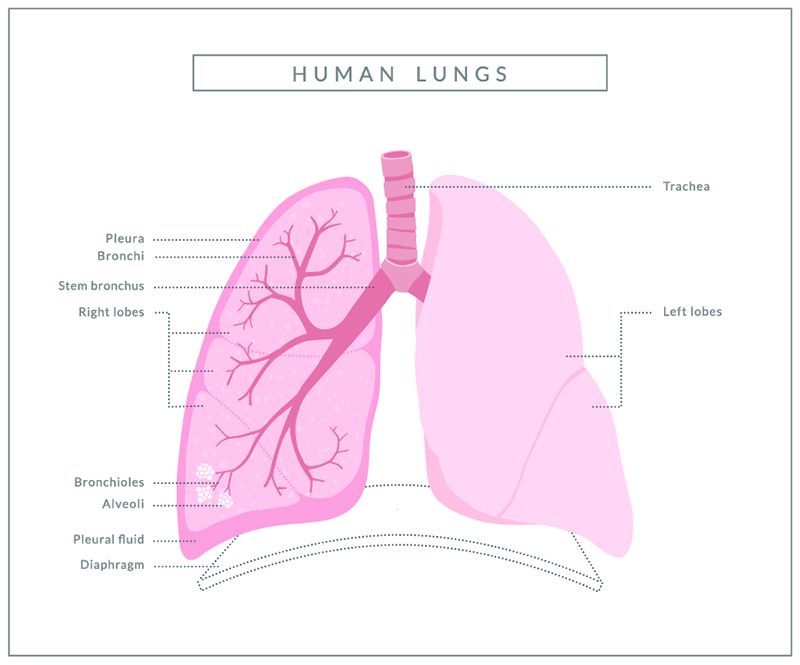
Dr Murphy: Healthy lungs are like big pink sponges. They're really quite sizable. So, if you think of the size of your ribcage, the lungs go from just above your collarbones or your clavicles in the base of your neck. All the way down to the bottom of your ribcage, one on each side.
Host: Your lungs sit inside your ribcage, there is one on the right and one on the left. The left lung is a little smaller because it shares that space with your heart. But, how exactly do your lungs help to deliver oxygen to the rest of your body? Dr Murphy explains that the lungs are designed a little like a tree.
Dr Murphy: I often describe them as thinking about them like a tree. So, you have your trachea or your windpipe and that's a little bit like the trunk of the tree. And then it goes down into the chest and it divides into two. So, there's an air passage called a bronchus that goes to the right lung and there's a separate one that goes to the left lung. And then they break further down into smaller pieces. So, the right lung has three lobes, or three parts, and the left lung has two. And within those parts, those little air branches are getting smaller and smaller and smaller as they go out towards the surface of the lung. They're so tiny, they're about the thickness of a hair. And you've got about 30,000 of those tinnier air passages called bronchioles.
On the end of those are tiny little air sacs that are called alveoli, and they're like little clusters of grapes. And all over the surface of them are tiny blood vessels called capillaries. And that's a really important part of your body because that's where all the action takes place in regard to absorbing the oxygen that you breathe in, in the air that crosses over through the alveoli and into those capillaries where it attaches to red blood cells and carries that oxygen out of the lungs, back through the heart, and around the body. It's also down on those alveoli and the capillary networks where the waste gases that your body has produced such as carbon dioxide get exchanged from the blood back into the air and you then breathe that out.
Outside the lung, there's a lining on the outside that's called the pleura. The pleura is a very important part of your lung. It allows the lung to slide within your chest cage. So, when you take a really big breath, and you'll feel that your ribs expand, that's the lungs actually getting bigger. And likewise, when you breathe out, the lungs are shrinking. And that pleural surface allows the lungs to slide and move really freely within your chest cage.
Host: Try it now. Place your hands on your ribs and take a big breath.
That’s the lungs getting bigger and when you breathe out, they get smaller. There's a muscle between your lungs and tummy, called the diaphragm. Which helps with this process, by contracting and relaxing each time you breathe.
Dr Murphy: The other thing that's going on is the passage of blood through the lungs, so your entire blood supply circulates through your lungs. And so, it leaves one side of the heart, circulates through the blood vessels in the lungs, and then it goes from the lungs back into the left side of the heart, and then out to the body to give the rest of your body oxygenated blood.
Host: As well as helping to deliver oxygen around your body, Dr Murphy says, the lungs also play a vital role in talking.
Dr Murphy: So, in your neck, you have something called your vocal cords, which is commonly called the voice box. And for you to be able to make sounds or phonate, you need to have air passing across the vocal cords and they move and vibrate and that's how you generate sound and words. And to be able to have that air move across your vocal cords it needs to come from within the lungs. So, to be able to speak you need to be able to take a deep breath. You need to be able to modulate or adjust the amount of air that you're breathing out through the vocal cords making them vibrate and producing a sound.
And likewise, the other important thing they do is they help you cough. And that's another really important thing in regarding to staying healthy.
Host: The lungs were one of the first organs to grow when you were inside the womb and as Dr Murphy explains, they worked a little differently before you were born.
Dr Murphy: When you're a foetus, and you're in your mother's womb, you are breathing amniotic fluid, and your body is designed to do that. And then when you are born, that fluid is expelled from the lungs. Some of it is sort of coughed out or breathed out. Some of it is absorbed by the body to empty those air sacs so then they can fill with air. And you have a special material inside those air sacs called surfactant, which enables them to open and not just collapse down on themselves. And that process happens when your baby is delivered, that the fluid is gone, and the air sacs filled with air. Likewise, the circulation in the baby changes as well. And there's a little duct that needs to close off to allow the passage of blood through the heart, and the lungs to change in a way that you need for life outside the womb. And it's an amazing process and all that happens after delivery.
One of the problems that happen when babies are born premature is that the lungs aren't ready to do that. They haven't got enough surfactant, that material that allows their little air sacs to pop open, and then stay open and fill with air.
Host: Our lungs begin to develop in the womb, but they aren't fully developed when we're born. In fact, they'll continue to grow alveoli, the little air sacs, right up until early adulthood.
Dr Murphy: After early adulthood, though, unfortunately, with age, all of our cell lung function gradually declines, but not normally to the point that it causes any problems except in settings of disease. So, for people who, for instance, have diseases like asthma that might not be well treated or people who smoke or people who are in very polluted environments, they might have an accelerated decline in that normal decline in lung function, and therefore end up with symptoms much younger than you would otherwise.
Host: Enjoying this episode? Be sure to tell others by leaving a rating or review in your podcast app or sharing that you're listening on socials!
Are you ready for this episode's mystery body part? See if you can guess the body part from the clues given. We'll reveal the answer at the end of the episode.
Usually I'm the biggest of the group, but not always.
I provide additional leverage when walking.
If I get bumped, you'll be in a lot of pain.
If you have, hallux limitus, you may have trouble bending me.
Do you know what I am?
There are lots of different diseases that can damage your lungs. Dr Murphy talked us through some of the common conditions that can affect Queenslanders.
Dr Murphy: The different diseases affect different parts of the lung. So, the air passages, so they're like the trunk and the branches of the trees, the diseases that can affect that. The common ones are asthma, and also chronic bronchitis are the most common that affect the air passages.
Host: Asthma is a chronic lung disorder that causes airways (the tubes that carry air in and out of the lungs) to become inflamed, which means that they swell and produce lots of thick mucus.
Dr Murphy: The best treatment for that is an inhaled therapy, so a medication that you breathe in. So, everyone would have heard of Ventolin, which is a drug called Salbutamol that helps relax the air passages and open them up. And that's a common treatment that we use for asthma. There are lots of other inhaled therapies or puffers is probably the common term for them that deposit medication on the air passages and allow it to relax and open up those air passages so people can breathe more freely.
Host: If you'd like more information about Asthma, we've included a helpful video explainer in the show notes.
Dr Murphy: The diseases that affect the lung tissue, which are a little bit like the leaves on the trees and the alveoli in the lung are things like infection. So, pneumonia is the medical term for an infection in the lung tissue itself. And so, the lung tissue doesn't work, and it gets filled up with the infection and lots of fluid and white cells that are trying to fight the infection. But that's one of the reasons why patients who have pneumonia get very breathless and often have trouble with oxygen because those air sacs are all clogged up and can't work properly.
The other thing that affects the air sacs is emphysema. So, emphysema is usually associated with smoking though there are some other causes. And what happens is those air sacs are destroyed and you end up essentially with holes in the lungs, and that's what emphysema is. But the other thing that emphysema does is it makes the lungs bigger than they should be, and bigger is not better. So, people who have emphysema where their lungs are really quite hyper inflated or larger than they should be. It's like taking a really deep breath and holding it but feeling like that all the time. And that's a very uncomfortable way to be.
Host: Dr Murphy says there's no cure for emphysema but there are treatments to help manage the condition.
Dr Murphy: There is no real treatment foremphysemaonce you've got it you can use inhalers that might help the air passages but the actual holes in the lungs, once you've developed those, you're going to have those forever. It doesn't mean you shouldn't stop smoking; you should definitely stop smoking to stop them getting bigger and deteriorating. But once those holes are there, it's like having a scar in the lung and they're not really ever going to go away.
Host: While your lungs might not be able to heal scars, they can mend themselves in other ways that are pretty impressive.
Dr Murphy: You've got a lot of reserve when it comes to your lung function. So, if you have two healthy lungs, you could have one of those lungs removed and you will be okay living with one lung. It is true that the remaining lung will expand. It doesn't expand to be the same size as things would have been if you still had two lungs, but the other lung that's remaining will expand to a degree.
Host: So, if one lung is removed, the other can actually grow bigger to help you breathe. But what happens when one or both of your lungs collapse? Can they be inflated again?
Dr Murphy: Pneumothorax means that your lung has collapsed. It can collapse because there's a hole in the lungs. So, air is leaking out of the lung and around, and that's a pneumothorax. And that air can't get out. So, it's got nowhere to go. It's sort of trapped. And if the hole persists and air continues to leak then you have to really allow that air to be evacuated some way and the way you do that is to put in a small drain called a chest tube.
With the pneumothorax there's really three groups. The first group is traumatic. So, people who've had an injury to the chest, they've broken ribs. That can put a hole in the lung and lead to a pneumothorax. The other two are either spontaneous primary pneumothorax or spontaneous secondary. And the difference is in people who've got a spontaneous primary pneumothorax they don't have a diagnosed underlying lung disease. So, they're otherwise often really young, well, fit people. The classic sort of what we call a phenotype or description of the patients is they're often very tall slim men.
Host: We spoke with Josh, a young Queenslander, who's suffered a collapsed lung not once, but twice.
Josh: Hi, my name's Josh. I live in Brisbane. And I'm a 35-year-old male.
Host: Josh explains that leading up to his first spontaneous pneumothorax, or collapsed lung, he had bronchitis and had recently gone diving but the symptoms set in at the gym a couple of weeks later.
Josh: I was at the gym doing some deadlifts, and I think at about the top of the fifth rep cycle I felt some pressure behind my sternum. And so, I immediately dropped the weight, sat down on the floor, and the head coach came over and sort of wanted to know what happened. So, I sort of explained to him and said, "Look, I'm having shortness of breath, and I've got some pain behind my sternum." And he, not being a doctor, just gave me some advice and told me just to relax and breathe it out for a little bit, thinking it might've been just something to do with cartilage or something else, and say. The pain didn't really go away, and I was down there about 45 minutes.
Host: The next day, he decided to go to the doctor because he wasn't feeling any better. And, after receiving a referral to get an x-ray, he discovered he had a collapsed lung.
Josh: I went straight into it to get an x-ray, and yeah, they advised me that I had a collapsed lung, and to go to the hospital immediately.
From that point, yeah, they had told me sort of what had happened, and advised me of the next sort of steps that I could do, which was to have a tube inserted into the pleural space of my lung to try and fix that issue.
Host: He said finding out his lung was collapsed was a shock, but it was also a relief to find out what he was feeling was real.
Josh: I kind of knew how I was feeling, which was a little bit abnormal. So, hearing the advice, I was relieved in a way that it was something kind of serious and it wasn't just something that I was making up. But also, yeah, fear did set in once I guess the reality of it was that I did have a collapsed lung, and them instructing me to go to hospital immediately, it was quite scary.
Host: Remember what it felt like when we asked you to take those deep breaths? Now, take that deep breath again but imagine you can only get halfway. It doesn't make you feel good, does it? It might make you feel lightheaded or panicky.
Josh: It's a strange feeling. It feels like somebody is treading on your chest, and you can only breathe a quarter of what you used to kind of breathing. I guess that's probably the easiest way to explain. There is some pain, and I think once the initial kind of onset passes, it really is just a matter of the shortness of breath that you're kind of struggling with from that point on.
Host: The procedure to remove the trapped air on the outside of Josh's lungs hurt a little more than he'd expected. This is because the pleura, the lining on the outside of the lungs, is very sensitive.
Josh: It was quite painful. So, them telling me what they were doing seemed okay and I was comfortable with that. They did administer the local anaesthetic around the area, so where they would insert the tube. And they did say they'd been inserting this tube into, and they showed me an x-ray of where they would be inserting that. And essentially once the drain's put in there, that allows your essentially lung to push the air out that shouldn't be there and reinflate to a point where it's stuck to the rib lining again.
But what they didn't tell me was, I guess when the tube goes in, that whole area is still very sensitive, and I don't think they can target pain relief for that area. So, I guess, yeah, it did actually feel like I was being stabbed, and there was nothing that they could really do to ease that pain. And so that tube was in there for about 12 hours, and it just felt like there was a knife in me the entire time.
By the following morning they'd done a few scans and some tests, and it was showing signs that it was reinflated. So, they essentially took out the tube, stitched me up, and told me not to lift anything heavy or overexert myself for about six weeks. And that's pretty well the advice that they told me. No more scuba diving or anything sort of to put you at risk of it happening again. And really at the time it was only the diving that they reinforced that I can't do.
Host: Josh was told that there was a risk that it could happen again, and it did. It was 8 years later when he was again working out at the gym on his lunch break when he suddenly felt that same pressure in his chest.
Josh: I had just put the weights back on the rack and then I went over to the water bottler to get a drink. And I started feeling a little bit of pressure behind the sternum again. I thought it was maybe I hadn't warmed up enough, and maybe it was just that I'd strained something somewhere on my lungs or back or something.
The first thing that went through my mind was, "My gym sessions done today. I'm just going to go back over and unpack the weights and call it a day." Within about 30 seconds, I found myself having to sit down on the floor.
So I had my back against the wall, taking some very shallow breaths, and I'd sort of caught the attention of the staff at the time and waved them over. And they came over and asked me what's happened, and I told them that, "Look, I think I've got a collapsed lung." Told them about my prior history, and they jumped on it straight away, called the ambulance. And within about 10 minutes, I had the ambulance there to check my vital signs and blood pressure and everything and initiated the process again.
Host: When his lung collapsed the first time it was only a quarter of the lung but this time it was over half and the doctors were concerned that the collapsed lung was pushing on his heart.
Josh: They were talking about surgical procedure straight away. And both my wife and I were a little bit scared, I guess, of the surgical sort of procedure and we wanted to see if the drain would work first. So, we kind of convinced them to do that initially, and that was showing some positive signs. The lung was starting to bounce back a little bit.
And so, we ended up leaving the tube in, it was almost a week in the end, and they were monitoring that on a day-by-day basis, taking an x-ray every day. And it got to about day four, maybe day four or five, and it stopped inflating. It kind of hit this point where it just wouldn't improve any further.
Host: They decided to perform a thoracoscopy, a surgical procedure where a video camera is inserted into the chest, to see why the lung wasn't reinflating. And, while they were there, they performed a pleurectomy, removing the lining of the lung.
Josh: They performed a thoracoscopy through keyhole surgery. And I think they did about three incisions. Went in with some cameras initially to look around and try to assess the area and try to identify the issue. From that point, they then used the same holes to, I guess, perform the procedure. And that was they pulled back the outer lining of my lung, and it all sounds fairly gruesome, but they pulled back the outer lining of the lung. So, it causes inflammation of the lung, and that makes that service very, very sticky. And then as the lung is reinflated, and I think they did provide some assistance during surgery to reinflate the lung, once the lung touches the rib lining, and again, it more or less forms a permanent bond. And so that was the surgical procedure that they did. And by the next morning I was, I was feeling much, much better even.
And so the way they tell that it has worked and that your lung has sealed up again is that they have a little machine that detects if there's any air coming out, and it blows air into this chamber full of water, and so that creates bubbles. So, every time you exhale, if there are any bubbles in there, it meant that you were losing air. So pretty much for a little while there I was still blowing bubbles, which meant that I had an air leak. But then that quickly went away.
And then once they were satisfied with that, they took the tube out, and I didn't have any anaesthetic. It was quite quick and pain-free. They pulled the tube out, and then they stitched up, it's almost like about a centimetre, I guess, the hole that's left behind, they stitch it up, and that's it. Went home that afternoon.
Host: Like many Queenslander COVID-19 has probably consumed your thoughts and life for most of 2020. And while it has been linked to the flu because it also affects your respiratory system, Dr Murphy explains it's a little different.
Dr Murphy: COVID-19 is a virus as you all know, and so I think most people know about the flu virus, but COVID-19 is a little bit different. It's very contagious.
The way you contract COVID-19 is you need to be exposed to the virus on one of your mucous membranes. So, they the surface of your eyes, or the lining of your nose and your throat, and the lining of the lung. And the way that can happen is if someone who has the virus cough or sneezes on you. But equally important, the other way it can happen is if you touch surfaces that are contaminated with the virus, and then you touch your face or your eyes. And so, the virus attaches to the mucous membranes, invades the cells, and then begins to spread. So, it's like the virus, it is really like an invader. It gets into the cell. It takes over the cell. It makes more virus, and then it spreads to adjacent cells.
And because it gets into the body through the respiratory system, it gets down inside the lungs where it causes a lot of irritation and a lot of inflammation. And the body's response to that in trying to kill off the virus using your immune system is it causes more swelling in the area. So what can happen in the lungs is that the cells in the lungs are very damaged, but they're also very swollen, and that leads to a lot of extra fluid in the lungs. And that stops the lung functioning because the lung is meant to be a sponge full of air, and it's like a soggy sponge if it gets full of fluid. That makes you very breathless. It will make you cough, and very importantly, it means that the oxygen levels in your blood will be very low because that network of the lungs where it's meant to pick up oxygen can no longer work because the air sacs are now full of fluid.
Host: If you'd like to know more about how our immune system responds to COVID-19 listen to our immune system episode.
You can't live without the lungs. So, how do you look after them?
Dr Murphy: There's quite a lot we can do to keep our lungs healthy. So, everyone knows I'm going to tell people not to smoke. So just start with that one. It's never too late to quit smoking. Ideally, people would never start. It's a very, very addictive habit. But if you have started, it's never too late to quit. Because when you do quit whilst you'll have age related decline in your lung function, you won't have the accelerated decline that happens related to ongoing exposure to tobacco smoke. Smoking marijuana and e-cigarettes will also cause damage to the lungs and reduce your lung function over time. So, not smoking is really important.
Host: Exercising regularly and having good nutrition can also play a role in keeping your lungs healthy. But Dr Murphy explains that it's not about being skinny.
Dr Murphy: Nutrition, so you don't want to be too skinny, but you don't want to be overweight because that puts extra load on the lungs. So, focusing on good nutrition and maintaining a healthy weight is very important. Vaccination is also very important. So, flu vaccination in particular, but there's another vaccination called pneumovax, which protects against the most common type of pneumonia with a bug called pneumococcus. And so, some age groups, particularly the elderly, and the very young should also be vaccinated against pneumococcus.
Host: Dr Murphy cares for a variety of patients, some who spend a short amount of time with her and others who require on-going care. She says both aspects of her job are equally rewarding.
Dr Murphy: So I think there is three bits I like about my job. The first thing is I love looking after people who are just really sick and getting them better. So, people who have really terrible pneumonia, that's a lung infection, and managing them, and seeing them get better, and then watching them leave hospital. I really get a lot out of that process. But equally, I really like getting to know my patients over a long period of time. So, I've been in this job for more than 15 years, and there are some patients that I've looked after for 15 years. So, I've known them a really long time, and we develop a really lovely relationship. And I really, really enjoy that aspect of respiratory medicine as well. But the third thing I like is I work in a big public teaching hospital, and I really like teaching and educating the next generation of doctors. And also, the next generation of nursing staff and allied health staff as well.
Host: Thanks for joining us for this episode of My Amazing Body. Before we go - did you guess the mystery body part? If you've ever stubbed your hallux, then you've stubbed your big toe! Congratulations if you figured it out.
Thank you to Dr Michelle Murphy and the team at Metro South Hospital and Health Service for telling us all about the lungs and thanks to Josh, for sharing what it's like have a collapsed lung. My Amazing Body is brought to you by Queensland Health. Many thanks to my colleagues: Lauren and Jess our producers, Carol our sound technician and Helen on music and sound effects.