 You’ve probably heard the term ‘ambulance ramping’ before. But what is it exactly, and why does it happen?
You’ve probably heard the term ‘ambulance ramping’ before. But what is it exactly, and why does it happen?
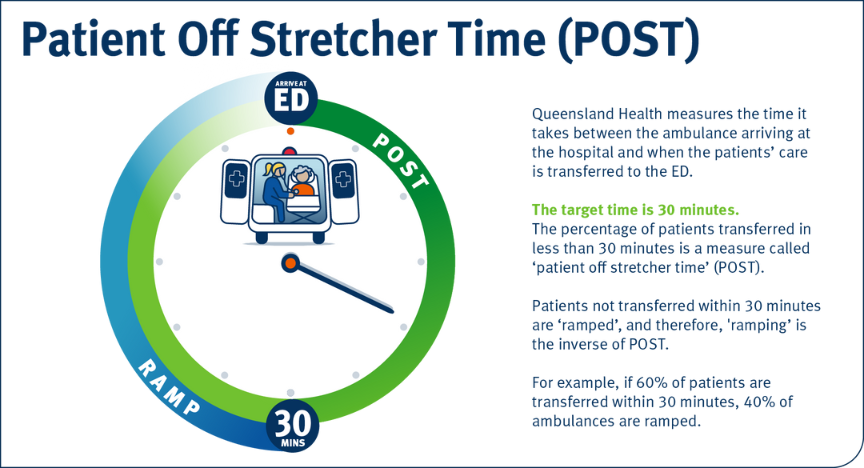
When a patient is taken to hospital in an ambulance, their care is transferred from the paramedics in the ambulance to the doctors and nurses in the emergency department (ED).
If this transfer doesn’t happen within 30 minutes of the ambulance arriving at the hospital, the ambulance is ‘ramped’. It does not mean the patient is still in the back of the ambulance, just that the transfer of care from paramedics to the ED clinicians has not yet happened.
On arrival to our hospitals, no patient is ever without care—either from a paramedic or ED doctor or nurse—and even at Queensland’s busiest EDs, all Category 1 patients with imminently life-threatening conditions are seen immediately.
But demand is increasing faster than population growth. Patients are presenting with more complex and chronic conditions. Access to residential aged care and disability care is not keeping pace with demand. Costs of private healthcare is rising, and many Queenslanders are struggling to access primary care.
- How ramping happens
- The emergency department
- Triage and treatment
- Admission or discharge
- Patient flow
- Bed block
- Surge capacity (also referred to as load sharing)
- What can be done?
- Keeping emergency for emergencies
- Interjurisdictional comparison
How ramping happens
Ramping occurs when patient flow through a hospital is impeded and is reflective of whole-of-hospital pressures.
This means patients arriving at EDs via ambulance cannot be transferred into the ED’s care in a timely manner.
For a patient to be admitted from ED to a hospital ward, a bed must first be available.
If all the beds are occupied with patients who require ongoing care, then the patient is unable to leave ED.
If this continues, it can result in a backlog of patients in ED waiting for a bed to become available, which means ED has no space to accept new patients that present to ED.
The result is ambulance ramping.
Patient flow is the term used to describe a patient’s journey through the hospital system from arrival at ED to admission to a hospital ward and discharge home.
Optimising our processes throughout the entire patient journey from admission to discharge is essential to ensure timely, effective, and high-quality care and to avoid ambulance ramping.
Ambulance ramping is not a new phenomenon; it occurs around the world, including in places with highly advanced health systems, such as Australia.
Before we look further into what ramping is, it’s helpful to understand how a patient moves through the hospital, from when they arrive to when they are well enough to leave.
The emergency department
An emergency department (ED) is a busy part of a hospital where patients who need urgent medical attention for severe injuries or illness go, without an appointment.
People may need to go to ED for severe or urgent conditions like heart attacks, severe pain, loss of consciousness and problems with breathing or bleeding.
The ED also treats injuries from accidents and other incidents, such as broken bones, drug overdoses and severe burns.
Patients can get to an ED on their own or via an ambulance when they call Triple Zero (000).
About one-third of Queenslanders use an ambulance to get to an ED. They are dispatched by the Queensland Ambulance Service—the largest and busiest ambulance service in Australia. In fact, Queensland is the only mainland Australian state that has a free ambulance service, increasing the number of people who use the service.
When someone comes to ED with a serious injury or illness, they are triaged by specially trained staff to determine how quickly they need care. From there, staff will treat and start their care as needed.
The ED has treatment areas called bays, where doctors and nurses treat patients in a medical emergency.
If a patient arrives at the ED by ambulance, and there’s an ED bay available, the paramedics transfer care of the patient to the ED doctors and nurses.
If no bays are available, paramedics will continue to care for the patient until one becomes available.
It’s important to note that on arrival to our hospitals—even in instances of ambulance ramping—no patient is ever without care, either from a paramedic, or ED doctor or nurse
Emergency medical treatment is free to Medicare cardholders at Queensland public hospitals.
Triage and treatment
Most Queensland public hospitals have an ED that is open 24 hours a day. Patients can arrive at any time and with any medical condition.
On arrival, staff will check how serious a person’s condition is.
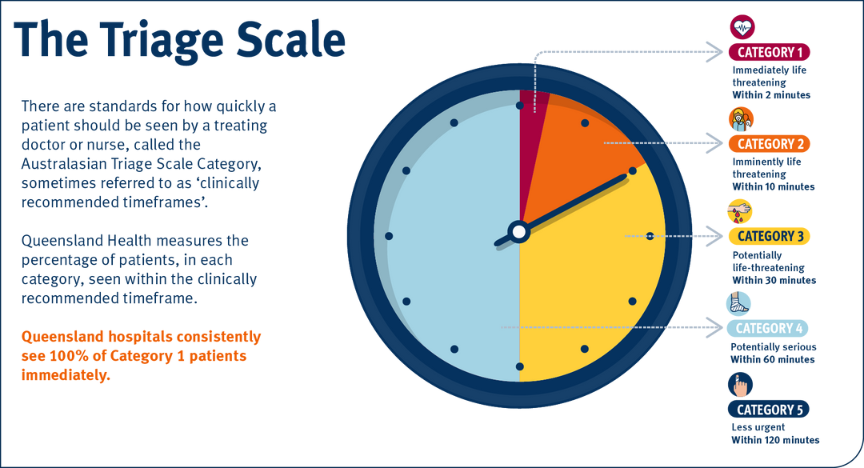
In Australia, EDs use a triage system, which ensures the people who need help most urgently are treated first.
The triage system has five levels:
- Category 1 – needs treatment immediately
- Category 2 – needs treatment within 10 minutes
- Category 3 – needs treatment within 30 minutes
- Category 4 – needs treatment within 1 hour
- Category 5 – needs treatment within 2 hours.
EDs are busy places. Doctors and nurses treat patients according to the severity of their condition, not when they arrived or whether they came by ambulance.
This means the sickest patients are always seen first.
It also means that patients with less serious conditions may need to wait, especially when the ED is very busy. Sometimes, those patients in categories 4 and 5 might wait several hours.
No patient is ever without care. Even at Queensland’s busiest EDs, all Category 1 patients with imminently life-threatening conditions are seen immediately.
Watch this video for a quick explanation of how triage works in an ED.
Admission or discharge
After receiving free medical treatment in the ED, a patient can either be admitted or discharged.
If the patient needs more treatment in the hospital, they’re admitted and moved to a hospital bed in another area of the hospital (a hospital ward).
If the doctor decides the patient is well enough to leave the ED, they’re discharged and can go home, sometimes with a plan to see a GP or specialist later.
Patient flow
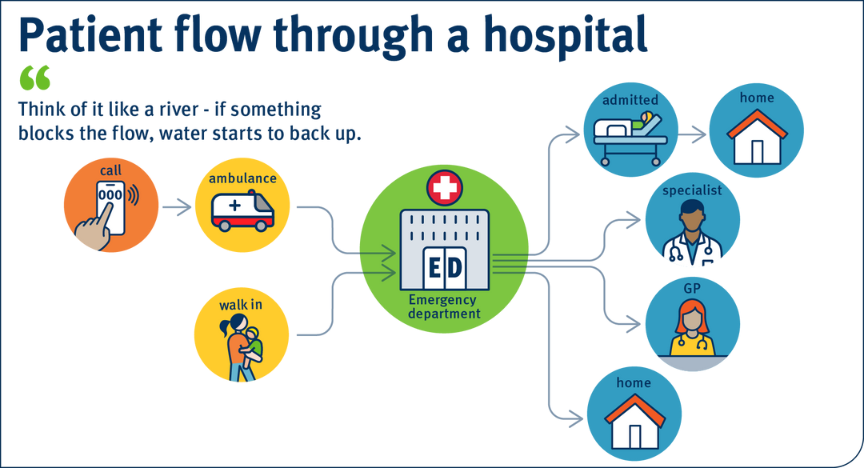
It can be helpful to think of a typical patient’s stay in hospital as a journey—from the ED to a hospital bed in a ward, and finally, discharged to go home.
If this flow is disrupted at any point, it can cause problems in the whole system. Think of it like a river—water starts to back up if something blocks the flow.
Put simply:
If patients aren’t or can't be efficiently discharged from hospital, they stay in ward beds.
When all the ward beds are full, patients can't come in from the ED. This means that ED patients who need a hospital bed stay in the ED and can cause a backlog.
If ambulances can't transfer new patients to the ED, they become ramped.
Bed block
Bed block is a term used to describe the problem that leads to ambulance ramping.
It refers to a blockage in the hospital system that affects the flow of patients.
There are various reasons for bed block, but the most significant contributor to this issue is long-stay patients.
These patients who are medically ready for discharge—that is, they no longer need to stay in hospital—but cannot leave as they don’t have a residential aged care bed, an aged care support package or a disability support package that would allow them to live safely in the community.
As of August 2023, there were 877 long-stay patients in our hospitals, which is equivalent to the number of beds across the Rockhampton, Toowoomba, and Redcliffe hospitals.
Surge capacity (also referred to as load sharing)
Hospitals plan for periods of high demand, but even the best planning doesn’t ensure unlimited ED treatment bays, hospital beds and staff.
Sometimes, things happen suddenly, like an outbreak of disease or a big accident, which means lots of people need help at the same time.
In Queensland, our hospitals function as a network. If one hospital is experiencing high demand, ambulances may transport patients to other nearby hospitals, but only if it is safe for the patient.
What can be done?
The Queensland Government is working to improve healthcare by addressing the challenges of ambulance ramping and bed block. This includes building new hospitals and expanding existing facilities to increase the capacity of the public health system.
An important part of this strategy is the introduction of new services like Minor Injury and Illness Clinics (MIICs) at our Satellite Hospitals and Medicare Urgent Care Centres. These services provide free, walk-in urgent care for those who need medical attention but can’t get an appointment with their GP. They treat conditions that aren’t life-threatening, such as simple fractures and infections, toothaches, and minor burns.
These initiatives are improving healthcare accessibility and providing prompt medical attention for non-life-threatening emergencies.
Non-urgent (Category 4 and 5) emergency department presentations decreased by more than 13 per cent in locations where satellite hospitals are operating (Caboolture, Kallangur, Ripley, Redlands, and Tugun).
In addition, West Moreton, Wide Bay, Sunshine Coast, Metro South, Metro North, Mackay, Darling Downs and Central Queensland HHSs are receiving a combined $9.1m. This will be used for:
- ED access nurses: Increase the availability of nursing care in EDs with a focus on triage and waiting room nursing support. This will allow the faster transfer of patients from ambulances to the care of EDs during peak presentation times (7 days a week).
- ED waiting room nurse: enhance waiting room safety to reduce patient risk during peak presentation times (7 days a week) by:
- Monitoring patients in the waiting room and escalation of patient care when required.
- Medical commanders: Funding dedicated senior doctors to act as ‘medical commanders’ managing the flow of patients from ambulances to the emergency department. This will enable early senior medical assessment of all patients.
Keeping emergency for emergencies
So, what can you do to help?
Each year, almost 1 million emergency department cases are not medical emergencies and could have been treated by a General Practitioner (GP) or pharmacy instead.
Part of easing the pressure on our health system is accessing the right care for your situation.
Only call Triple Zero (000) for an ambulance or visit an ED in an emergency medical situation.
If you’re not sure if your medical condition requires emergency care, call 13 HEALTH (13 43 25 84). Registered nurses are available 24 hours a day. They will advise you on what to do and if you need to go to a GP, pharmacy or ED.
For less urgent or less serious conditions, always visit a GP. They treat many general conditions such as viruses, infections, removing stitches, UTIs, sprains, earaches and much more.
Pharmacies can also help with conditions such as cold and flu symptoms, skin conditions and irritations, minor or mild allergy symptoms, headaches, diarrhoea or constipation, and sleeping problems.
Satellite Hospitals and Medicare Urgent Care Centres are available across Queensland for treatment of urgent care that isn’t life-threatening. These are open 7 days a week, free for Medicare card holders and don’t require an appointment.
Find a health service that’s closest to you.

Interjurisdictional comparison
There is no consistent national measure for the recording or reporting of ramping; meaning each state has their own differing method of measuring performance. These differences can include what constitutes the ‘start’ and ‘end’ times of ambulance transfer times, the types of transfers which are included or excluded from the reporting datasets and even the target timeframe for transfers to be completed within.
Despite having the busiest ambulance service within Australia, when applying the methods used by other states to Queensland’s data, Queensland’s performance was found to be better than three of the five comparable jurisdictions. As per the latest publicly available reporting period for each jurisdiction, Queensland outperformed these jurisdictions by a margin between 3.6 and 16.6 percentage points. Whilst for one further jurisdiction, the performance differential was reduced significantly.
On the whole, Queensland’s Emergency departments are performing well when compared with other jurisdictions, reporting the second-best median wait time (18 minutes) and the second largest proportion of patients seen within clinically recommended timeframes (67 per cent) in the 2022-23 fiscal year – performing better than the national average in both metrics.