Summary
This episode is part of the It Can’t Hurt to Ask: In My Blood podcast
In this episode, learn all about how blood works. We’ll be answering questions like what is blood made of? How does your body stop bleeding after a cut or scrape? Why are blood tests so important? Do people really have more blood in their body when they’re pregnant?
Featured in this episode

Dr Aarya Murali
Dr Aarya Murali is a haematology registrar employed through Pathology Queensland at QML Pathology. A haematology registrar is an expert in blood diseases, and in this episode, Dr Murali takes us through the basics of how blood works.

Dr Jeremy Robertson
Passionate about what he calls the ‘essential elements of life’, Dr Jeremy Robertson has been studying haematology and related conditions for over 20 years now. He works at Queensland Children’s Hospital, treating children who have blood-related conditions.
Episode resources
Bone marrow
In this episode, Dr Murali talks about the role of bone marrow in the production of blood cells. Want to learn more about how bone marrow works? Listen to My Amazing Body – Bone Marrow, to find out all about it.
Circulatory system
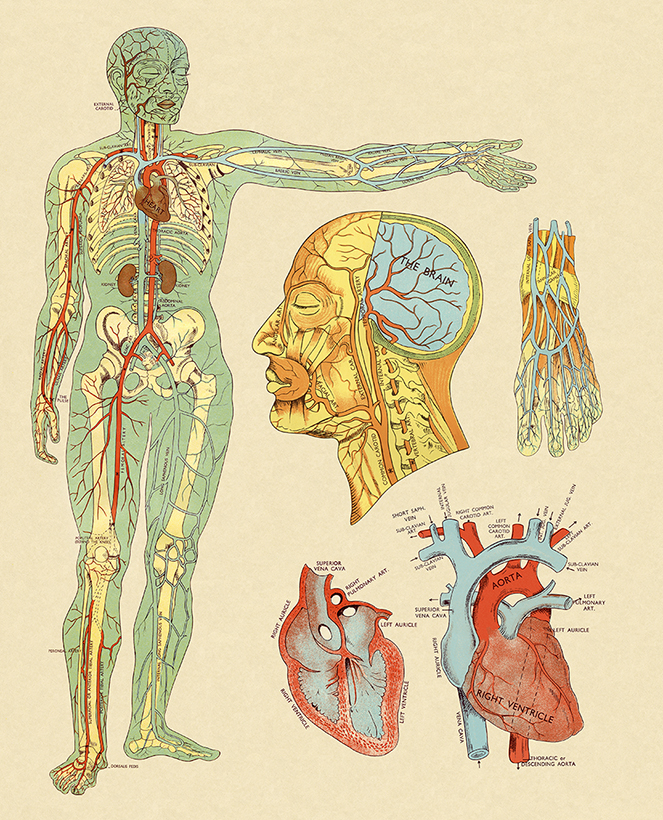
This diagram shows the circulatory system. In this episode, Dr Murali explains where and how blood travels as it journeys around your body.
Blood and bleeding disorders
In this episode, Dr Murali and Dr Robertson talk about different types of bleeding and blood disorders and the symptoms they cause. You can find out more about blood and bleeding disorders from Health Direct and Lifeblood.
How blood tests work
In this episode, Dr Murali explains how blood tests work, and what happens to your samples at the pathology lab. You find out more about what to expect from a blood test and how to prepare from Health Direct.
Transcript
Vox pops: What is blood made of?
How does our body stop itself bleeding?
Why are blood tests so important?
Do I really have more blood in my body when I'm pregnant?
Narrator: When it comes to our health, everyone’s got questions or curiosities. From shower thoughts to conversations with family or friends, where do you go to learn more?
From Queensland Health, It Can’t Hurt To Ask is the new myth-busting health podcast with the answers.
With no such thing as a silly question, each episode will explore an interesting health topic, speaking to top experts and everyday people to share facts and tips to better understand your health, inside and out.
Hi, I’m Lauren and welcome to the very first episode of It Can’t Hurt To Ask, recorded on the lands of the Jagera and Turrbal people. We acknowledge the Traditional Custodians and pay our respects to the Elders past, present and emerging.
As always, whatever you hear in our episodes is general information. Always speak to your doctor about your individual circumstances.
Let’s get into it, shall we?
This season, the theme is ‘In My Blood’. Each episode you’ll hear from a variety of voices as we explore a blood-related health topic; think blood donation, mosquito-borne viruses, blood cancers and conditions, periods, blood sugar and much more.
Today, we’re starting at the very beginning. What is blood, why does it matter and how does it work?
We’ll hear from two experts today, Dr Murali and Dr Robertson, who are both haematologists. Hematology is the study of blood and blood disorders, making them the perfect people to answer our questions!
Even as young children, we’re fascinated by the idea of blood. In the playground, our cuts and scrapes bleed, dry out and get picked at, over and over. That led to questions from a young age about what exactly is going on in our body … and why is it red?
Dr Murali: My name is Aarya Murali and I'm a hematology registrar employed through Pathology Queensland, currently working at QML Pathology.
So, in its most basic sense, blood is made of cellular elements and non-cellular or fluid elements, if you like. And there are many different types of cells in blood, but you could divide them broadly into three main categories.
You have your red cells that help you carry oxygen to the rest of your body. You have your white cells that help you fight infections. And then you have your platelets that are very important to make sure that you don't bleed excessively or that you can stop bleeding when you cut yourself or you know to prevent internal bleeding and so on.
Narrator: Sounds like a dynamic trio, right? And what about what’s in those fluid elements?
Dr Murali: The fluid component of blood consists partly of water but of course also electrolytes and various minerals and they also have various proteins in it. And there are again, a whole raft of these proteins.
You know, you've got things like albumin, which are really important for making sure the fluid stays within your vascular system and that balance is appropriate. You have various clotting factors that again, help to make sure that you stop bleeding if you cut yourself and help to protect against things like internal bleeding.
And then you have proteins like your immunoglobulins, which are very, very important in helping you fight infection.
So, it's a very, very complex system that all interacts and work together to maintain health and function in an individual.
Narrator: Wait, but what makes our blood red exactly?
Dr Murali: Essentially the red colour in blood comes from this substance or protein called haemoglobin. And haemoglobin is actually present within the red blood cells. And it consists of haem, which has iron within it, and globins and it's because of this substance, this protein called haemoglobin, that actually helps to pick up oxygen from the lungs and deliver it to tissues. It is this substance that gives blood its red colour.
Narrator: If you hadn’t realised just how essential and far-reaching our blood system was, you’re hopefully starting to now. Yet, pardon the platelets, we’ve still only just scratched the surface.
So, let’s go deeper, to the very source. To the part of the body that actually makes your blood cells. Any guesses where that might be?
Dr Murali: The cellular components of blood are primarily made within your bone marrow. And in the adult, your bone marrow is you know, sort of the spongy inside of your bones, and that's predominantly in your pelvis, your breastbone or your sternum, and also in your vertebrae. And that's where most of the blood in your body is produced, the blood cells.
Once they're produced, and they're in circulation, there are, you know, different processes that happen for their maturation. But once they’re mature blood cells in circulation, and they sort of travel through the body in a very, you know, linear fashion, if you like. So, it's sort of a circuit.
Narrator: Like many bodily parts and processes, as an automated system a lot of this work goes on without us even knowing or thinking about.
So, let’s join it for one loop, shall we? Hop in, seatbelt on and keep your hands in the cell carriage at all times, please.
Dr Murali: So, say we're starting at the right side of the heart. What happens is, on the right side of the heart, you've got your right atrium and your right ventricle. And usually blood starts, say in the right atrium, it travels into your right ventricle. And from your right ventricle, it's pumped into the lungs. Now in the lungs, that's where the blood actually picks up the oxygen that you breathe in. And also the carbon dioxide that the blood carries with it is released out into the lungs at the same time.
Then the blood cells move from the lungs into the left side of the heart and first enters the left atrium, then it travels into the left ventricle and then from the left ventricle it's pumped out to the rest of the body. And it's pumped out through these big blood vessels known as arteries and the blood travels through the arteries, goes into these smaller blood vessels called capillaries, which infiltrate the various cells and tissues and organs.
And at this capillary level, the blood is able to then release the oxygen that it has carried with it from the lungs into these tissues. It's able to take up some of the waste that is produced as part of normal metabolic processes in these tissues, and then is able to travel back through veins back into the right side of the heart.
And this whole circuit starts again. And if you estimate an average heart rate of 70 beats, this process happens about 100,000 times a day.
Narrator: 100,000 times a day. Do you feel dizzy just thinking about it? All this going on while we’re working, eating, sleeping…
But if we do pay attention, are there signs we can see or feel what is going on?
Dr Robertson:
Hi, I’m Jeremy Robertson. I’m a paediatric haematologist at Queensland Children’s Hospital.
Narrator: Passionate about one of the essential elements of life, Dr Robertson has been studying haematology and related conditions for over 20 years now.
Dr Robertson: Pulse is the beat that you feel in your wrist or in your leg each time the heart pumps blood. So that little bub-bub-bub feeling in your wrist is actually a pulse of blood going past in an artery. That's one way of actually feeling what the circulation is doing.
Narrator: Ok, be honest. Were you trying to feel your own pulse just then? Me too. The easiest way to do it is to put out one of your hands, palm-side up. Take your first finger and middle finger on your other hand and place the pads of those fingers on the inside of your wrist, lined up with the base of your thumb. Press gently and you should feel your pulse.
Dr Robertson: We also sometimes have an awareness of our heart beating. If that's very strong awareness, we call that a palpitation. But a lot of the time, if you're exercising or if you're nervous, you feel your heart racing and that's normal because the heart is a large muscle and so you feel it moving inside your chest and you may even feel the pulses of blood going up into your head, particularly when the heart's beating faster.
Narrator: Another important function of the blood system is temperature regulation. Turns out how our body changes when we’re hot and cold has a lot to do with our circulation.
Dr Robertson: We can see the effects of circulation also with changes in activity or in temperature.
So, you know, we all know when you exercise or it's a hot day, your cheeks go red. That's the blood vessels in the skin getting larger to help cool the blood down. And similarly in the cold, people will often notice their fingers will go sort of slightly white and pasty and will feel cold and for some people that effect is very pronounced. Again, that's the circulation actually constricting blood vessels, making them tighter, sending less blood to the small blood vessels in the skin to try and preserve temperature centrally.
So in addition to the functions of delivering oxygen, fighting infection and getting all those proteins and fluids moving around the body, the circulation also has a critical role in regulating temperature and that's probably our best day-to-day awareness of the circulation doing anything apart from of course when you cut yourself or graze your skin and you see bleeding then you know obviously that's a much more visible example of blood. Most of the time though, we don't see it.
Narrator: Now we know how our blood and its systems are designed to work, we can also appreciate the impact they have when they’re not working.
Dr Murali: So going through the cellular elements of blood, for example, if someone has reduced red blood cells within their body, that essentially means that they're not able to deliver oxygen to their tissues. And that is to every single tissue in the body, to every single organ in the body.
And so essentially what that means is your oxygen delivery to organs such as your kidneys, your brain, your heart, that will all be compromised, to varying degrees, of course, depending on how severe the reduction in your red blood cells is.
Similarly with white blood cells, very, very important in fighting infection. There are a whole different groups of white blood cells and they're all, you know, they all have slightly different functions and are effective or important in different aspects of immunity. But as a sort of an overarching principle, if you've got very, very low white blood cell count, your body is at an increased risk of infection.
And without or with critically low platelets, you're at risk of bleeding, bleeding from your nose, bleeding from your mouth, and bleeding in more dangerous locations like inside your brain and inside your gut as well.
If there are problems with protein elements such as albumin, then that essentially affects how the fluid volume or the fluid component of blood is distributed. And so, you can have imbalances and people can have problems like fluid overload and so on and so forth.
Similarly, if you are low in clotting factors or you're low in immunoglobulins, then that can affect your ability to clot and also fight infection.
So, it's a really crucial part of maintaining just everyday health and function in every individual.
Narrator: As part of his work at Queensland Children’s Hospital, Dr Robertson and his team see and care for young patients with many different blood disorders and conditions. These can range from mild to more severe.
Dr Robertson: In our clinic, we see a lot of children with a tendency to bleed. So, diagnosing bleeding disorders is a large part of our job. Bleeding disorders are individually rare but as a group are fairly common. The reassuring thing for people to know is that most children who seem to bruise easily or seem to be a little bit of a bleeder don't have an underlying bleeding disorder.
Bleeding disorders include very severe bleeding disorders like haemophilia, but also milder bleeding disorders like Von Willebrand disease. These fancy names are all traditional names. They come from historical terms, either people who've discovered the conditions or old terminology. For example, haemophilia. Haemo is just Latin for blood, and philia is to like so Haemophilia is meant to be a tendency to blood.
Narrator: Von Willebrand disease is actually quite common, impacting about 1% of the population.
Von Willebrand factor is the name for a large protein that helps your platelets to stick to blood vessels when you’re bleeding. It’s kind of like glue, to create a clot and hopefully stop the bleeding.
So, if your von Willebrand factor is lacking or not working as it should, it means your blood can’t clot properly.
Dr Robertson: So, it's an important clotting protein. Lowish levels can give you a tendency to bruise and have other types of bleeding symptoms like nosebleeds. And that condition is probably the most common bleeding disorder that we see. And thankfully, most people, it's quite mild and doesn't require any day-to-day management. It's more just planning around procedures and basic first aid.
Narrator: So, that’s one of the most common and often mild bleeding disorders. Other blood-related conditions Dr Robertson and his team see are inherited blood conditions; conditions that are passed down genetically. One of the best known of these? Thalassemia.
Thalassemia is an inherited condition within your genetic code in your haemoglobin. Remember, that’s the protein that’s in your red blood cells. It means that you are either producing a reduced quantity of alpha or beta globins, or a different or a variant type.
To have a child with thalassemia, both parents have to be carriers.
Dr Robertson: The carriers themselves don't have any awareness of being a carrier but it is picked up on routine blood tests. So often it is known that parents are carriers before a child is born.
If both parents are known to be carriers of thalassemia or sickle cell disease, there's a one in four chance of having a child with a clinically significant disorder, either of thalassemia or sickle cell disease.
Narrator: As very severe conditions, symptoms often present early with diagnosis either during pregnancy or in early infancy.
Dr Robertson: Alpha thalassemia is so severe that it typically presents in the womb. So, it's diagnosed often at 20 weeks when you have your standard morphology scan that the foetus is already showing signs of having severe anaemia.
Beta thalassemia and sickle cell disease often don't present until infancy or later in the first year of life and that's because in the womb most of our haemoglobin is what's called foetal haemoglobin, which is slightly different to adult haemoglobin.
And that transition from foetal to adult haemoglobin happens gradually over the first three to 12 months of life. And when that occurs, the effects of beta thalassemia or sickle cell disease become apparent.
So, beta thalassemia typically presents somewhere around four to six months of age with very significant anaemia, problems with growth, enlarged organs because the organs are trying to make more blood and can't.
Narrator: When it comes to diagnosing disorders and conditions in our blood, the first step is usually a blood test. These are ordered by your doctors as part of a clinical assessment which could be part of a general health check-up or to work out why you’re experiencing certain symptoms.
There are many different types of blood tests. Some might look at the quantity of red or white blood cells. Others might look at how your organs are functioning or where your cholesterol levels are sitting.
One of the most common tests you might experience is called a full blood count. This is a very informative test that provides information on your haemoglobin levels and the different types of cells in your blood, the quantity and whether that’s normal for your age and gender.
Dr Murali: So, for example, if your doctor orders a full blood count, you would typically come into a collection centre. You'll have your blood taken if you are an outpatient, usually by one of the phlebotomists.
Narrator: Hold up, a phlebotomist? Yep, that’s the official term used for someone who is professionally trained to take blood from a patient. Back to Dr Murali.
Dr Murali: And there are specific requirements in terms of, if it's this test that's being ordered, it needs to be collected into this tube and so on. So usually a phlebotomist will, as you may have experienced, they'll check your name, your date of birth, do all of that paperwork side of things. They'll check what tests have been requested. They'll get the tubes that are required for those tests ready. Then they'll usually collect that sample, usually from a vein in your arms, that's placed into the tube. That tube is then labelled and then those tubes, along with the request form with the test, are taken to the lab.
Once it arrives at the lab, it's a very, very complex system with lots of checks and balances in place to first of all make sure that we're releasing accurate results and we're releasing them in a timely manner to your clinician and actually giving your clinician the information that they've asked for from that particular test.
So, once it gets to the lab the tests are divided up, the tests are then, depending on how the exact test is done, it would be placed on an analyser or a machine that can perform that test.
Once that test is performed by the analyser, a set of results are sort of released or given by the analyser to the scientific staff in-house.
Now if we have a really grossly abnormal result or an unexpected result, usually, you know, that's where we start troubleshooting and that's, you know, usually involving the scientists as well as the doctors that work within the lab such as myself.
And we try and work out, well, is this result abnormal? Why is it abnormal? Is this a problem with the sample or with that particular collection. Is this a true result?
If it's true, what are the implications of that? And if it's a grossly abnormal result, then usually, and it's a time critical result, usually someone from the lab will also be in touch with your doctor to let them know that this is a time critical result that needs to be actioned.
Narrator: Different tests require different amounts of blood. If you’re having multiple blood tests, then it might need to be put in multiple tubes. And interestingly, the actual tube is important too.
Dr Murali: The tubes that we actually collect the blood in, they actually contain various sort of additives and anticoagulants just to preserve that blood and to make sure that it is transported in an optimal condition to allow for that testing to occur.
Narrator: Anticoagulants are chemical substances that prevent your blood from undergoing coagulation or solidifying to form a clot. Ethylenediaminetetraacetic acid—thankfully more commonly referred to as EDTA—is an anticoagulant that is commonly used within the tubes that full blood count is collected in. It ensures the blood is preserved in the best way possible to be tested when it gets to the lab.
If you’re preparing for a blood test, it’s always best to ask your doctor if you need to do anything specific beforehand. Some common requirements can be too fast, to ensure an accurate estimate of certain levels of things in your blood, or to stay well hydrated so they can find your veins relatively easily.
Narrator: To finish off, let's have a myth-busting question submitted by you.
Voxpop: Do I really have more blood in my body when I'm pregnant?
Dr Murali: The answer is yes. So, the fluid component of blood, the plasma component, goes up by about 30 to 50%, and then your red blood cells actually expand by about 20 to 30%, so not quite as much, but still expands.
And that's because obviously you've got more, you know, physiological demand in pregnancy because you also have to provide oxygen and nutrients to the developing foetus and that additional sort of top-up helps assist with that.
Narrator: There you have it. After all, it can’t hurt to ask.
What a journey it’s been. We’ve followed our blood cells right from creation in the bone marrow to the tips of our fingers as it regulates our temperature. We’ve heard how blood tests actually work, how our body heals cuts and stops bleeding and some of the common blood disorders we see in Queensland hospitals.
And it’s just getting started. In the coming weeks, we’ll be learning more about blood and organ donation, why our blood sugar matters, mosquito-borne viruses, antibodies and much more.
New episodes drop every Wednesday.
If you enjoyed this episode, please rate or review. Even better, tell or share with a friend, family member or colleague who you think would also enjoy it.
Until next time, bye bye!