Statewide Anaesthesia and Perioperative Care Clinical Network (SWAPNet) Sugammadex injection 200mg in 2mL and 500mg in 5mL
Guideline number: QH-GDL-442:2023
Effective date: 1 June 2023
Review date: 1 June 2026
Supersedes: new guideline
- Statement
- Purpose
- Scope
- Requirements
- Human Rights
- Auditing
- Supporting Documents
- Approval and implementation
- Version Control
1. Statement
Residual neuromuscular blockade is a common phenomenon that has been identified as a significant risk factor for adverse postoperative patient outcomes1.
Sugammadex (trade name Bridion®) is a selective relaxant-binding agent that is designed to encapsulate rocuronium and chemically similar steroidal muscle relaxants such as vecuronium.
The main advantages of Sugammadex when compared with conventional anticholinesterase agents are much faster reversal and the unique ability to reverse rapidly and efficiently, for the first time, deep levels of neuromuscular blockade.
It has been shown that even with unrestricted availability of Sugammadex in a large Australian hospital residual neuromuscular block was not able to be completely abolished1. As such where there is concern about the possibility of residual neuromuscular blockade, the use of a quantitative neuromuscular transmission monitor is highly recommended.
Sugammadex is a relatively high cost medication that has the potential to significantly impact drug expenditure and its usage should be monitored.
Anaesthetists must recognise that there are alternatives that can be used when the clinical situation dictates.
2. Purpose
This guideline provides recommendations to support the appropriate management of the use of Sugammadex injection 200mg in 2mL and 500mg in 5mL in Queensland Health facilities.
It is accepted that:
- The use of Sugammadex is regulated but not prohibited.
- The Queensland anaesthetic community promotes an evidence-based approach to the use of Sugammadex.
- Individual departments develop local practice to monitor the use, storage and audit of Sugammadex.
3. Scope
This guideline applies to all Queensland Health employees (permanent, temporary and casual) and its agents (including visiting medical officers and other partners, university and other healthcare provider staff and students, contractors and consultants).
4. Requirements
Sugammadex demonstrates clinical advantages in patients with pulmonary disease, cardiac disease, hepatic dysfunction, myasthenia gravis and / or morbid obesity over standard reversal with neostigmine and glycopyrrolate (Drugs 2016:76(10)1041). However, given the current cost implications and paucity of research supporting the cost effectiveness of widespread use, it is not recommended as the standard reversal agent for all cases and its use should be restricted to specific indications only.
The use of Sugammadex in the reversal of neuromuscular blockade by rocuronium or vecuronium in Queensland Health public hospitals is restricted to the following indications:
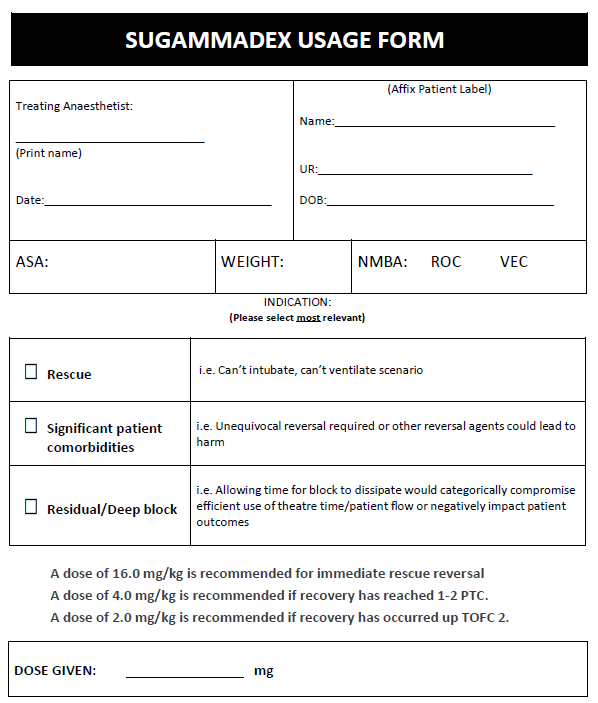
- Rescue: as rescue therapy in ‘can’t intubate, can’t oxygenate’ situations
- Significant Patient Co-morbidities: when significant comorbidities mandate the unequivocal reversal of neuromuscular blockade (eg. neuromuscular disease, severe respiratory or cardiovascular disease, morbid obesity) and / or the anticipated physiologic effects of other reversal agents could reasonably lead to patient harm (eg. cardiovascular disease and concern about instability with neostigmine and/or glycopyrrolate and/or atropine)
- Residual / Deep Block: when a patient’s depth of neuromuscular blockade is either not suitable for reversal or has been incompletely reversed with standard agents and allowing time for neuromuscular blockade to dissipate would categorically compromise the efficient use of theatre time / patient flow, or negatively affect patient outcomes.
4. Human rights
Human rights are not engaged by this guideline.
5. Auditing
The use of Sugammadex should be subject to local controls developed by individual departments of anaesthesia. It is recommended that the collection of local audit data at each facility be undertaken to monitor usage, cost and safety. Other information considered for auditing should include dose, indication for use and any suspected adverse events. An example of an audit form is attached.
6. Supporting documents
Economic evaluations reveal that Sugammadex may lead to significant resource savings within the hospital setting, however well-designed independent analyses from the Australian perspective are lacking (1-11).
Downloadable PDF: Sugammadex injection 200 mg in 2mL and 500mg 5mL guideline
- Milne J, Ong C, Cheung K, Schauer A, Buttar S. The influence of introducing unrestricted access to Sugammadex and quantitative neuromuscular monitors on the incidence of residual neuromuscular block at a tertiary teaching hospital. An audit of ‘real-life’. Anaesth Intensive Care 2016:44;6:784.
- CADTH Rapid Response Reports. Sugammadex for the Reversal of Neuromuscular Blockade in Adult Patients: A Review of Clinical Effectiveness and Cost-Effectiveness. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health.
- Keating GM. Sugammadex: A Review of Neuromuscular Blockade Reversal. Drugs. 2016;76(10):1041-52.
- Abad-Gurumeta A, Ripolles-Melchor J, Casans-Frances R, Espinosa A, Martinez-Hurtado E, Fernandez-Perez C, et al. A systematic review of sugammadex vs neostigmine for reversal of neuromuscular blockade. Anaesthesia. 2015;70(12):1441-52.
- Brueckmann B, Sasaki N, Grobara P, Li MK, Woo T, de Bie J, et al. Effects of sugammadex on incidence of postoperative residual neuromuscular blockade: a randomized, controlled study. British journal of anaesthesia. 2015;115(5):743-51.
- Carron M, Baratto F, Zarantonello F, Ori C. Sugammadex for reversal of neuromuscular blockade: a retrospective analysis of clinical outcomes and cost-effectiveness in a single center. ClinicoEconomics and outcomes research : CEOR. 2016;8:43-52.
- De Robertis E, Zito Marinosci G, Romano GM, Piazza O, Iannuzzi M, Cirillo F, et al. The use of sugammadex for bariatric surgery: analysis of recovery time from neuromuscular blockade and possible economic impact. ClinicoEconomics and outcomes research : CEOR. 2016;8:317-22.
- Ledowski T, O'Dea B, Meyerkort L, Hegarty M, von Ungern-Sternberg BS. Postoperative Residual Neuromuscular Paralysis at an Australian Tertiary Children's Hospital. Anesthesiology research and practice. 2015;2015:410248.
- Martinez-Ubieto J, Ortega-Lucea S, Pascual-Bellosta A, Arazo-Iglesias I, Gil-Bona J, Jimenez-Bernardo T, et al. Prospective study of residual neuromuscular block and postoperative respiratory complications in patients reversed with neostigmine versus sugammadex. Minerva anestesiologica. 2016;82(7):735-42.
- Olesnicky BL, Traill C, Marroquin-Harris FB. The effect of routine availability of sugammadex on postoperative respiratory complications: a historical cohort study. Minerva anestesiologica. 2016.
- Unal DY, Baran I, Mutlu M, Ural G, Akkaya T, Ozlu O. Comparison of Sugammadex versus Neostigmine Costs and Respiratory Complications in Patients with Obstructive Sleep Apnoea. Turkish journal of anaesthesiology and reanimation. 2015;43(6):387-95.
7. Approval and implementation
| Guideline Custodian | Contact Details | Approval Date | Approver |
|---|---|---|---|
| Executive Director, Healthcare Improvement Unit | HIU@health.qld.gov.au | 1 June 2023 | Executive Director |
8. Version Control
| Version | Date | Comments |
|---|---|---|
| V4.0 | 3 February 2017 | Endorsed by SWAPNet Steering Committee |
| V5.0 | 1 June 2023 | Endorsed by the SWAPNet Steering Committee |