Variable life adjusted display and other national patient safety indicators guideline
Guideline number: QH-HSDGDL-032-1:2013
Effective date: 11 March 2024
Review date: 11 March 2027
Supersedes: Version 2.0
On this page:
- Purpose
- Scope
- Guideline
- Supporting and related documents
- Approval and implementation
- Version control
- Appendix 1 VLAD indicators and flagging levels
- Appendix 2 VLAD business process map guideline
1. Purpose
This Guideline supports and provides recommendations to Hospital and Health Services (HHSs) regarding best practice for meeting the Patient Safety Health Service Directive’s mandatory requirements for reviewing and reporting on Variable Life Adjusted Display (VLAD) and other National Patient Safety Indicators (National PSIs).
2. Scope
This Guideline applies to Queensland Health employees, agents, volunteers, contractors, consultants and managed service providers working for the Divisions within the Department of Health, Agencies and Business Units and for the Hospital and Health Services (including Visiting Medical Officers).
3. Guideline
VLAD – description and background
- VLAD is a screening tool applied to clinical indicators to assist in identifying potential areas of concern, or strengths to improve patient safety and quality of care. VLAD attempts to improve Queensland Health’s understanding of causation and to determine whether corrective action is necessary.
- VLAD involves a flagging process which occurs when a pre-specified level of variation is reached, as measured by three Flagging levels (see: Table 1 below). When a VLAD flag occurs at a particular point, it suggests that over time there have been more (or less) patients experiencing the outcome than expected, up until the particular patient. The way to view this graph is to initially look for flags and then look backwards from the flagging point to identify the patients to review.
Table 1: Flagging levels by indicator group and level of variation
| Flag level | Variation from the state average | ||||
|---|---|---|---|---|---|
| Group A indicators | Group B indicators | Group C indicators | Group D indicators | Group E indicators | |
| Level 1 | 30% | 50% | 75% | 100% | 100% |
| Level 2 | 50% | 75% | 125% | 125% | 150% |
| Level 3 | 75% | 100% | 150% | 150% | 200% |
Note: A complete listing of indicators and groupings are in Appendix 1: VLAD indicators and flagging levels
- Flagging levels can occur at both an upper or lower level. An upper flag (for example level 3) indicates that a hospital’s outcome rate is lower than the state outcome rate whereas a lower level flag (for example level 1) indicates the hospital rate is higher than the state outcome rate.
3.1 VLAD review model
- VLAD is a quality monitoring tool and should be interpreted as such. It is designed to flag issues for HHSs for further review.
- The occurrence of a flag should not be immediately interpreted as indicating good or bad performance. This is because there are many possible explanations as to why the VLAD has flagged, one reason being simply chance.
- Where review is initiated, it is recommended the Pyramid Model of investigation be adopted (see: Figure 1). The Pyramid Model of investigation recommends a hierarchical approach to identify causation. Under this Model, factors at the base of the pyramid are more likely to be causes than factors at the apex.
Figure 1: Pyramid model of investigation

3.2 VLAD graphs and notification reports
- VLADs are generated on a monthly basis by Patient Safety and Quality (PSQ), Clinical Excellence Queensland (CEQ), Queensland Health using Queensland’s hospital admitted patient data, and perinatal data. Any delay in the submission of data from hospitals influences the currency of VLADs. VLADs are published via the VLAD Clinical Monitoring System (VLAD CM).
- Access to VLAD CM requires approval from the relevant HHS VLAD Authorising Officer (VAO).
- A monthly notification report listing new flags is sent by VLAD CM via email to the Chief Executive of the relevant (HHS CE), VAO, VLAD Hospital Coordinator (VHC) and other authorised users of VLAD CM. The notification report will also list overdue VLAD responses.
3.3 Notification report flagging rules
- In the case of multiple flags triggered for the same indicator in the same reporting period, only the highest level flag is notified to the hospital via a notification report, as this review will include findings for subordinate level flags.
- In the case of a new flag and a higher level flag in the previous reporting period, the new flag will not be notified to the hospital in the notification report, as it is expected the investigation for the earlier higher level flag will be thorough and include most of the cases that would be considered in a new investigation.
3.4. Response
- In response to a VLAD notification report a hospital is required to conduct a review and submit a response detailing all aspects of the review considered including details of cases reviewed, any issues identified and an action plan to correct an unfavourable result or to maintain a positive result.
3.5. VLAD levels requiring a response
- Mandatory
- As described in the Directive, lower level 3 Flags require a review and response submitted within 30 calendar days.
- Recommended
- Lower level 1 and 2 Flags and all upper level flags do not require a review to be undertaken.
- These Flags will be included in the notification report as non- reportable flags for a month following release.
- A review into these Flags may identify opportunities for improvement leading to a reduction in the likelihood of progression to a lower level 3 Flag. The VLAD CM information system will allow the submission of a response to these flags.
3.6. National Patient Safety Indicators
Hospitals with statistically significant variation against National PSIs are required to submit a review response to PSQ.
- National PSIs include the performance indicators published by the Australian Institute of Health and Welfare, and form part of The Australian Health Performance Framework [1]. The Department of Health monitors indicators aligned with the national indicators including the following:
- Hospital standardised mortality ratio - quarterly
- Death in low mortality diagnosis related groups – quarterly
- In-hospital mortality rates for specific conditions – monthly using VLAD
methodology - Unplanned hospital readmission rates for specific conditions – monthly
using VLAD methodology.
- PSQ will notify HHSs when a significant variation has occurred and provide assistance in review methodology.
- It is recommended the VLAD review model in Figure 1, above is followed when undertaking an investigation into variation.
3.7. Timeframes for response
- As described in the Directive, a HHS should review and complete a response to a mandatory flag or National PSI within 30 calendar days of notification.
- The response should be approved by the VAO before being submitted via VLAD CM.
3.8. Lower level 3 response
- It is recommended that a lower level 3 review considers outcomes of previous reviews for the indicator.
- For example, all cases considered in previous lower level 2 reviews and lower level 1 reviews, (if undertaken) and subsequent cases leading up to the lower level 3 Flag should be considered for a lower level 3 review. Progress on action plans from lower level 2 Flags should also be reviewed and documented.
3.9 Lower level 3 VLAD and national patient safety indicators response and escalation
- All responses to lower level 3 Flags and significant variation against National PSIs are reviewed by the VLAD Committee [2] which meets on a monthly basis.
- The VLAD Committee clinically reviews responses for adequacy and action plans. If concerns are raised, the VLAD Committee will request further information or actions from a HHS to be reviewed at a subsequent VLAD Committee meeting.
- Where a VLAD and other response/s, or request for further information from a HHS has not been received, the following escalation strategy is employed:
- First request: forward a memorandum to the HHS CE, (cc the VAO).
- Second request: table the matter at the relationship management meeting
- Third request: brief the Director-General – attach a memorandum from the
Director-General to the HHS CE.
- Issues unable to be resolved by the VLAD Committee are escalated to the Deputy Director-General, CEQ, Department of Health.
If a lower level 3 Flag is solely attributable to a structure or resource related issue, the VLAD Committee can approve that a hospital will not be required to undertake a review and submit a response for the lower level 3 Flags within the subsequent 12 months.
3.10. Suggested responsibilities—Department of Health
Table 2: Suggested responsibilities
| Role | Responsibilities |
|---|---|
VLAD Committee |
|
Systems team PSQ, CEQ, Department of Health (Systems Team) |
|
3.11. Suggested responsibilities—Hospital and Health Services
The following suggested roles and responsibilities in Table 3 should support the ability of HHSs to comply with the Directive and National PSI mandatory requirements.
(See also Appendix 2: VLAD business process map guideline which outlines a suggested process for coordination of the VLAD process within a HHS.)
Table 3: Suggested responsibilities
| Role | Responsibilities |
|---|---|
CE, HHS |
|
VLAD Authorising Officer (VAO) |
|
VHC |
|
Health Information Management Services Clinical Coder |
|
Clinician / reviewer |
|
4. Supporting and related documents
Authorising Health Service Directive
Patient Safety Health Service Directive QH-HSD-033:2014
Forms and templates
Appendix 1: VLAD Indicators and flagging levels
Appendix 2: VLAD business process map Guideline
5. Definition of terms used in this guideline
| Term | Definition / explanation / details | |
|---|---|---|
Variable Life Adjusted Display | A statistical methodology used to monitor patient outcomes to assist in identifying possible areas of concern or strength for safety and quality of care. It is to be interpreted and viewed with the intention to understand causation and to determine whether corrective action is necessary. | |
VLAD Clinical Monitoring System | An electronic information system that disseminates VLAD graphs, notification reports and captures HHS reviews/responses to VLAD flags. | |
Flag | A point on the VLAD, identifying a predetermined level of variation has been reached i.e. more (or less) patients have experienced an outcome than expected over a period of time. | |
Notification report | A list of new and previous flags that have occurred within a hospital requiring a VLAD response to be submitted | |
Response | Feedback from a hospital detailing what was considered in the review, review findings and actions | |
Systems Team | The Team within PSQ responsible for production of the VLAD graphs, maintenance of VLAD CM and the first stage review of VLAD responses. | |
National Patient Safety Indicators | National safety and quality indicators, managed by Australian Commission on Safety and Quality in Healthcare. |
6. Approval and implementation
Guideline custodian
Executive Director, PSQ, CEQ.
Approving officer
Deputy Director-General, CEQ, Department of Health
Approval date: 11/03/2024
Effective from: 11/03/2024
7. Version control
| Version | Date | Prepared by | Comments |
|---|---|---|---|
1.0 | 01/07/2013 | PSQIS | First issue |
2.0 | 31/01/2021 | PSQIS | Updated email addresses, phone numbers and the name Patient Safety Unit, to Patient Safety and Quality Improvement Service. |
3.0 | 22/01/2024 | PSQ | Updated Table 1 VLAD flagging levels by indicator group and level of variation, Appendix 1 VLAD indicators and flagging levels. Updated the name Patient Safety and Quality Improvement Services to Patient Safety and Quality. Minor administrative and clerical amendments. |
Appendix 1: VLAD indicators and flagging levels
| Flagging levels | Indicator and outcome |
|---|---|
| Indicator Group A (Flags triggered at 30%, 50%, 75% variation from state average) |
|
| Indicator Group B (Flags triggered at 50%, 75%, 100% variation from state average) |
|
Indicator Group C |
|
Indicator Group D |
|
Indicator Group E |
|
Appendix 2: VLAD business process map guideline
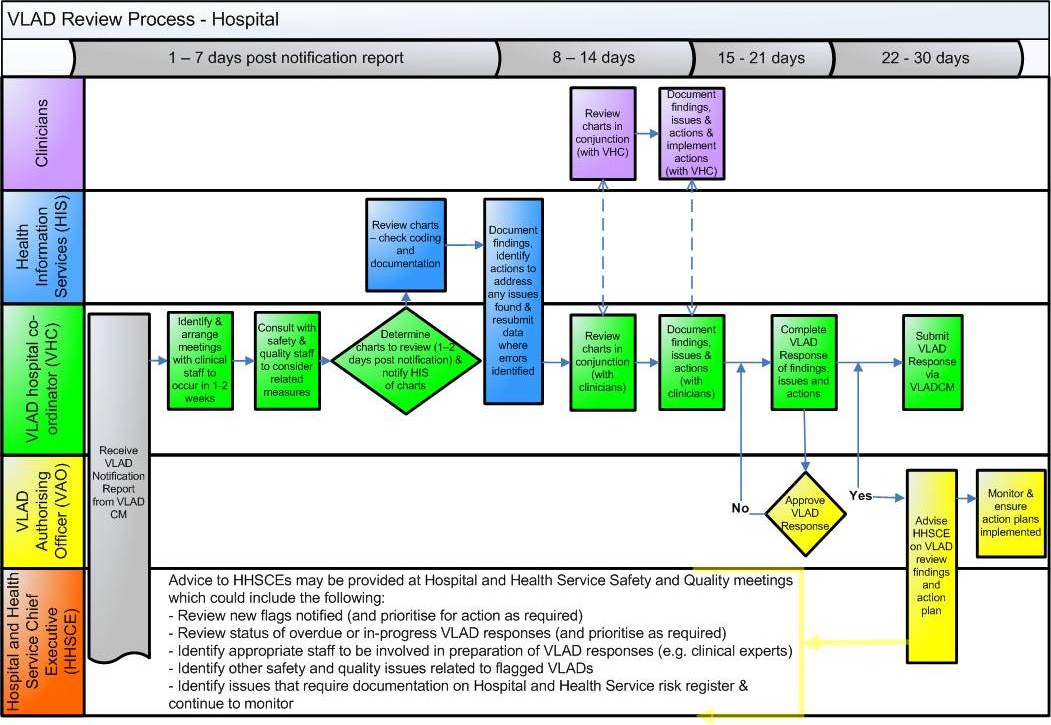
View larger review process image.
Footnotes
- The Australian Health Performance Framework accessible here: https://www.aihw.gov.au/getmedia/1c95574c-ac07-4126-8b7c-31eb29d9b381/OOS318_Attachment-1.pdf.aspx
- The VLAD Committee is a committee formed under the Department of Health.
PRINTED COPIES ARE UNCONTROLLED
CLASSIFICATION – OFFICIAL – PUBLIC