New or worsened confusion
This information does not replace clinical judgement. Refer to Conditions of use and copyright for further T&Cs.
New or worsened confusion may represent delirium, which is a sudden (over hours or days) change in a resident’s mental state with impaired attention and or altered conscious level and or impaired cognition, with severity of symptoms fluctuating or varying over the course of the day. It is important that staff are able to recognise new or worsened confusion and conduct an assessment that identifies the underlying cause of delirium and the complications associated with the new or worsened confusion.
Flowchart
The flowchart shows all of the information at one time. Health professionals should always remain within their scope of practice; these pathways should never replace clinical judgement.
Click the link below to view the full flowchart.
Practice points
The practice points are a systemised documentation of expanded relevant information - use only in conjunction with the flowchart - note, you can access each relevant point from the flowchart link.
-
Delirium is a sudden (over hours or days) change in a resident’s mental state with:
- impaired attention and/or
- altered conscious level and/or
- impaired cognition
- with severity of symptoms fluctuating or varying over the course of the day.
There are a number of subtypes of delirium that present differently.
Note: in mixed delirium, residents may move between hyper and hypo active delirium. There is acute onset of difficulty focussing attention and/or disorganised thinking, with: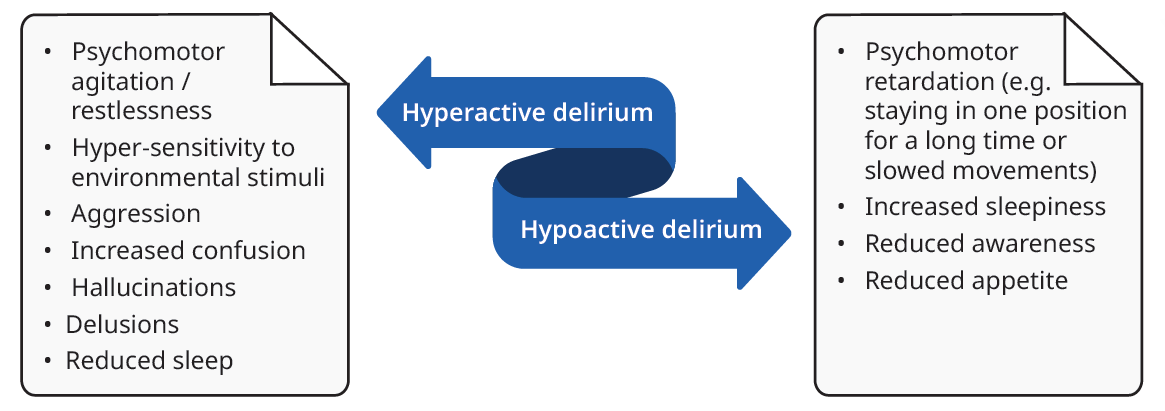
-
Goals of assessment are to:
- Confirm delirium.
- Identify the underlying cause of delirium.
- Identify complications of delirium.
Confirm delirium using a validated screening tool such as Confusion Assessment Method (CAM) or 4AT.
Identify causes of delirium using:
- History from the resident and carers (and family where appropriate and relevant).
- Perform an assessment of vital signs: where vital signs are unstable or cognition-appropriate pain assessment identifies severe pain, refer to the Management of Residents with Unstable Vital Signs Pathway to guide response.
- Review medication list for recently commenced or ceased medications.
- With GP, perform a head-to-toe examination to seek or exclude causes. The head-to-toe examination should be tailored to identify common causes of delirium sources of pain, urinary retention, infection, constipation, hydration status, trauma from recent falls, focal neurology. (See table below for guidance using a PINCHES ME pneumonic).
Identify complications of delirium including:
- Skin integrity check for pressure injuries.
- Falls with secondary traumatic injuries.
- Aspiration pneumonia where level of consciousness is altered.
- Dehydration and associated electrolyte abnormalities.
Delirium is associated with increased risk of persistent cognitive impairment and has an association with increased mortality, so response should be timely and concordant with a resident’s goals of care.
The table below outlines potential causes of delirium and related assessment actions.
Causes Actions Pain Perform cognition-appropriate pain assessment and where pain is present, identify location and likely source of pain - common sources of pain that may be easily missed include urinary retention, injuries from falls, pressure injuries Infection Look for sources of infection: examine chest, skin, abdomen for tenderness (suprapubic, flank, right upper quadrant), signs of meningitis Nutrition Screen for malnutrition using a validated tool e.g. Malnutrition Screening Tool Cardiac events Examine for evidence of heart failure; consider arranging ECG to look for myocardial ischemia Constipation Change to pattern or consistency of bowel motions Hypoxia Assess oxygen saturations, respiratory rate and examine chest (look, listen, feel) for causes of hypoxia Hydration Assess for evidence of dehydration Endocrine Check blood glucose level. Where indicated, check electrolytes, renal, liver and thyroid function tests Stroke Assess for focal neurological deficit (New onset of: Balance or co-ordination impaired; Eyes – reports of double vision or loss of vision; Facial droop, Arms can’t be raised or when raised, one drifts down, Speech slurred or unable to speak = Time critical) Medications Medication review for polypharmacy, recent additions (e.g. sedatives, anticholinergics or steroids), or recent cessation of medications associated with potential for withdrawal (e.g. sedatives, opiates) Mobility Recent falls or new change to mobility Environment Recent change to environment -
If any of the following red flags are identified in residents who have delirium, review the resident’s advance care plan, consult resident or substitute health decision maker (or nominated decision support person) and refer to Management of residents with unstable vital signs pathway. It is important to note that delirium may occur as a resident nears the last days or weeks of life. Management of delirium should consider the resident’s goals of care and life trajectory. The following are considered red flags in the resident with delirium:
- Vital signs in the red or danger zone including new severe pain - refer to Recognition of the deteriorating resident
- New drop in Glasgow Coma Scale or difficult to rouse relative to baseline
- New seizures associated with delirium
- New, painful bony deformity or hip pain with reduced range of motion or shortening/leg rotation
- Suspected head injury (witnessed head strike or clinical signs head injury in an unwitnessed fall) in a resident with a known bleeding disorder or on anticoagulant or anti-platelet agent
- New signs of a potential stroke (BE FAST: New onset of any of: Balance or co-ordination impaired; Eyes – reports of double vision or loss of vision; Facial droop, Arms can’t be raised or when raised, one drifts down, Speech slurred or unable to speak = Time critical)
Note: a decision to transfer a resident to hospital with delirium should always consider resident goals of care and be respectful of informed choice by the resident (or substitute decision maker). If the resident has a registered supporter, where possible the supporter should be included in discussions regarding a decision to transfer to hospital.
-
First screen for red flags as above. Where red flags are identified in residents with delirium, review the resident’s advance care plan, consult resident or substitute health decision maker (or nominated decision support person) and refer to Management of residents with unstable vital signs pathway
Escalate to HHS RaSS at GP discretion (or in terminal delirium to the resident’s palliative care provider) if any of:
- red flags in a resident who has conservative goals of care and does not wish to be transferred to hospital
- no underlying cause is identified in a resident with delirium
- resident has significant agitation or distress not responding to supportive cares and treatment of the underlying cause
- resident is not improving after 3 to 5 days despite implementation of supportive cares and treatment of the underlying cause
- resident has delirium associated with suspected alcohol withdrawal
- poor fluid intake and reduced urine output.
-
Residents with delirium require an individualised delirium care plan that includes:
- Treatment of the underlying cause of the delirium.
- Supportive care to minimise duration of delirium.
- Prevention and / or management of complications of delirium.
Treatment of the underlying cause: It is important to note that delirium may occur as a resident nears the last days or weeks of life. Where a cause is identified, ensure that management options (active treatment and/or a palliative approach to care) are discussed with the resident and their substitute health decision maker, to support informed choice. Treatment of reversible causes of delirium, may improve symptoms of delirium and this should be considered when developing a delirium care plan.
Supportive care should be implemented for residents with delirium regardless of goals of care. These supportive and risk reduction strategies may also be implemented to prevent delirium.
Note: pharmacological management of delirium (beyond treatments for the underlying cause) does not improve outcome. Where a person’s behaviours and distress pose an imminent risk to themselves or others, and non-drug methods have been implemented and failed, consult Therapeutic Guidelines: psychotropic for guidance on pharmacologic options. Antipsychotic medications for control of behaviours in delirium are a restrictive practice and there are legislative requirements for informed consent from the resident’s nominated restrictive practices substitute decision maker.Bundle of delirium supportive care and risk reduction strategies
A Assess, prevent and manage pain and constipation and regularly reassess B Best practice personal care: maintain hygiene and mouth cares, support toileting, maintain skin integrity (institute pressure injury prevention and daily skin moisturising for intact skin), sleep hygiene C Correct hypoxia and electrolyte abnormalities Communicate clearly and orient resident (verbal orientation, clock visible) Consistency of staff and environment D Drugs: cease anticholinergic drugs and reduce medication burden where this is clinically appropriate Deficits: address sensory deficits - ensure resident has their glasses / hearing aids available Diet and dehydration: where clinically appropriate, support oral intake, ensure resident’s dentures fitted, maintain hydration, monitor food and fluid intake E Encourage and support mobility and assist self-care Environment: diurnal lighting (access to natural lighting or ensure lighting follows day-night lighting), remove clutter that poses falls risk, low stimulus environment F Family engagement and empowerment to provide supportive care, reassurance and comfort Falls prevention plan
References
-
- NICE. Recognising and preventing delirium: a quick guide for care home managers2023 21 May 2023. Available from: https://www.nice.org.uk/Media/Default/About/NICECommunities/Social-care/quick-guides/Delirium-quick-guide-1-1.pdf.
- Chen X, Zhao X, Xu F, Guo M, Yang Y, Zhong L, et al. A Systematic Review and Meta-Analysis Comparing FAST and BEFAST in Acute Stroke Patients. Front Neurol. 2021;12:765069.
- Pryor C, Clarke A. Nursing care for people with delirium superimposed on dementia. Nurs Older People. 2017;29(3):18-21.
- Psychotropic Expert Groups, Therapeutic Guidelines: Psychotropic. Melbourne: Therapeutic Guidelines Limited; 2021.
- Dixon M. Assessment and management of older patients with delirium in acute settings. Nurs Older People. 2018;30(4):35-42.
- Wilson JE, Mart MF, Cunningham C, Shehabi Y, Girard TD, MacLullich AMJ, et al. Publisher Correction: Delirium. Nat Rev Dis Primers. 2020;6(1):94.
- Australian Commission on Safety and Quality in Healthcare. Delirium Clinical Care Standard. 2021. ACSQHC: Sydney. https://www.safetyandquality.gov.au/our-work/clinicalcare-standards/delirium-clinical-care-standard accessed May 2023.
- Woodhouse R, Burton JK, Rana N, Pang YL, Lister JE, Siddiqi N. Interventions for preventing delirium in older people in institutional long-term care. Cochrane Database Syst Rev. 2019;4(4):CD009537.
- Clinical practice guidelines for the management of delirium in older people. In: unit Ceahse, editor. Melbourne: Victorian Government Department of Human Services; 2006.
-
Pathway New or worsened confusion Document ID CEQ-HIU-FRAIL-60023 Version no. 3.0.0 Approval date 3/07/2023 Executive sponsor Executive Director, Healthcare Improvement Unit Author Improving the quality and choice of care setting for residents of aged care facilities with acute healthcare needs steering committee Custodian Queensland Dementia, Ageing and Frailty Clinical Network Supersedes New or worsened confusion Applicable to Residential aged care facility registered nurses and General Practitioners in Queensland RACFs, serviced by a RACF acute care support service (RaSS) Document source Internal (QHEPS) and external Authorisation Executive Director, Healthcare Improvement Unit Keywords New or worsened confusion, acute confusion, delirium, altered level of consciousness Relevant standards Aged Care Quality Standards:
Standard 2: ongoing assessments and planning with consumers
Standard 3: personal care and clinical care, particularly 3(3)
Standard 8: organisational governance