Dehydration and subcutaneous fluids
This information does not replace clinical judgement. Refer to Conditions of use and copyright for further T&Cs.
Dehydration is common in aged care and is associated with increased morbidity and mortality. Facilities should implement strategies to prevent dehydration including screening for hypohydration, staff education and tailored oral fluid intake plans. When dehydration does occur, early institution of an appropriate rehydration plan and management of underlying precipitants in a manner concordant with resident goals of care may prevent avoidable deterioration.
Flowchart
The flowchart shows all of the information at one time. Health professionals should always remain within their scope of practice; these pathways should never replace clinical judgement.
Click the link below to view the full flowchart.
Practice points
A systemised documentation of expanded relevant information - use only in conjunction with flowchart / decision tree above - note you can access each relevant point from the flowchart / decision tree link.
-
Goals of assessment include to assess hydration status and determine severity of dehydration, identify the cause of dehydration and to identify complications of dehydration.
A. Assess hydration status and determine severity of dehydration or volume depletion: No single clinical or laboratory feature reliably predicts dehydration in older adults.
Click here for information on assessment for dehydration or volume depletion1,2 (PDF 98 kB)
B. Identify the cause of dehydration:
Click here for common causes of dehydration in RACF residents (PDF 89 kB).
Where a cause of dehydration is not identified and does not resolve with simple therapy, in addition to GP review and where indicated, arrange screening for depression and cognitive impairment, swallowing evaluation, dental examination and a health assessment and medication review.
C. Identify the complications of dehydration:
Complications of dehydration include:
- Postural hypotension
- Decreased perfusion of vital organs:
- Acute kidney injury
- Delirium
- Worsening of underlying angina
- Fluid and electrolyte imbalance
- Increased risk of:
- Falls
- Renal stones
- Constipation
- Pressure injuries
- Mortality, particularly when dehydration is present in the setting of bacterial infection
-
Red flags for deterioration in residents with dehydration include:
- Severe dehydration
- Concurrent pulmonary oedema
- Terminal care or nearing end of life
- Coagulation defects
- Concurrent infection and sepsis
- Hyperactive delirium that may affect compliance with rehydration (oral or subcutaneous)
-
- Unstable vital signs (refer to Recognition of the deteriorating resident)
- Worsening confusion
- Syncope or concurrent falls
- Progressive worsening of dehydration rather than improvement
- Development of any of:
- Fever, infection or sepsis
- Pulmonary oedema or a new oxygen requirement (refer to Recognition of the deteriorating resident)
- Hyperactive delirium
- Chest pain
- Comorbidities that require stabilisation
- Acute on chronic renal impairment
- Electrolyte disturbance
- Lymphoedema
-
Where the resident appears clinically well and is assessed to have mild dehydration, oral rehydration should be considered in those who are able to swallow adequately.
Where dehydration is due to reduced intake, the resident should be encouraged to drink fluid in the form of drinks preferred by the resident e.g. hot or iced tea, coffee, fruit juice, water or sparkling water.
Where there is volume depletion secondary to diarrhoea or vomiting or is associated with deranged electrolytes, an oral rehydration solution is recommended. Where the resident appears unwell and is dehydrated, subcutaneous fluids should be offered in parallel with encouraging oral fluids.
Strategies to increase oral intake of fluids should be implemented including:
- High availability of drinks
- Offering varied choice of drinks, including drinks and temperature of drinks that are preferred by the particular resident
- Frequent offering of drinks - encourage residents to drink out of habit, not thirst as thirst is often blunted
- Staff awareness of the need for adequate fluid intake
- Staff support in assisting oral intake and in assisting in regular and timely toileting when required
- If thickened fluids are required and texture is appropriate, offer recognised foods such as custard and yoghurt first as these are often better accepted compared with unfamiliar thickened fluid
-
- Isotonic fluids (e.g. 0.9% saline) are indicated in mild to moderate dehydration where oral rehydration alone is not suitable. Note: necrosis of the skin may occur if inappropriate fluids are used
- The rate of administration of subcutaneous fluids should be individualised based on the degree of dehydration and resident comorbidities.
Generally, up to 60mL/hour is tolerated well, however caution is advised in those with a history of congestive cardiac failure or those on a fluid restriction or at risk of acute pulmonary oedema - Up to 2 sites may be used concurrently (e.g. 1L/day per site)
- For maximum absorption, rotate the site regularly (at a minimum after every 2L of fluid)
-
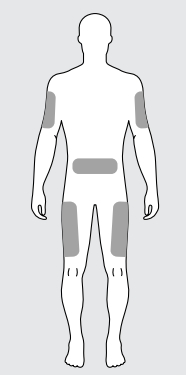
When selecting an appropriate site consider:
- Resident mobility and agitation
- Comfort and resident preference
- Accessibility for routine checks
- Skin condition
- Presence of adequate subcutaneous fat (e.g. 1.0 to 2.5cm of subcutaneous fat):
- anterior abdomen at least 4 fingers-breadth distant from the umbilicus; left iliac fossa is preferred due to increased distance between colon and the abdominal wall (avoid in residents with ascites)
- anterior thigh (avoid in residents with peripheral vascular insufficiency)
- upper outer arm (deltoid)
Avoid areas where skin has:
- Lymphoedema
- Bony prominences
- Prior exposure to radiotherapy
- Proximity to a joint
- Proximity to a surgical or wound site or tumour
- Evidence of infection or inflammation
-
- Insertion of subcutaneous access should only be performed by competent clinicians
- Use aseptic non-touch technique
- Perform skin antisepsis:
- use a single-use sterile applicator containing sterile alcohol-based chlorhexidine solution
- if the resident has an allergy to chlorhexidine, use povidone-iodine or 70% alcohol
- allow the product to dry naturally on the skin after application
- Use a small-gauge (24 to 27 G) and short-length non-metal cannula e.g. Teflon® or Vialon® cannula, such as BD Say-T-Intima® ) - these are associated with significantly less risk of site inflammation than metal butterfly needles
- Remove and insert new device at a new site if blood returns during device placement
- Secure using a transparent semipermeable membrane dressing to secure and allow observation and assessment
-
Monitor residents with dehydration closely including:
- Regular vital signs (frequency should be determined by severity of dehydration and underlying cause but should be performed at a minimum of once every 12 hours)
- Daily weight may guide adequacy of fluid replacement if baseline weight is known
- Oral or enteric intake
- Urine output - where a resident does not have a catheter
- Fluid losses e.g. diarrhoea
- Where subcutaneous fluids are used, the site should be checked every 4 hours for (and site changed if any of below identified:
- redness
- swelling or oedema
- bleeding / bruising
- leaking of fluid
- pain
- pooling or unresolved blanching
Where there is evidence of any of the above findings, the site of subcutaneous fluid administration should be changed.
- With GP review medication to access for need to with-hold or adjust dose of medications such as diuretics and antihypertensives
- Monitor for development of red flags or escalation criteria
- Skin integrity - implement two hourly pressure cares where indicated
- Maintain nutrition and monitor blood glucose level - arrange dietitian review where indicated
- Where resident has co-morbidities, monitor these to detect and address instability early
-
Ensure RACF has a strategy to reduce incidence of dehydration - example components of such a strategy may include:
- Screening for hypohydration by inspecting tongue for dryness prior to administration of medications - where identified, implement individual management plan to address
- Staff education to improve awareness of importance of adequate fluid intake and common causes of dehydration to residents
- Tailored oral fluid intake plans including:
- Ensuring high availability of a range of drinks at different temperatures and suited to individual resident preferences and swallow
- Teaching residents to drink from habit rather than only when thirsty
- Regular toileting to avoid resident anxiety about incontinence impacting fluid intake
References
-
- Broadhurst D, Cooke M, Sriram D, Gray B. Subcutaneous hydration and medications infusions (effectiveness, safety, acceptability): A systematic review of systematic reviews. PLoS One. 2020;15(8):e0237572.
- Gorski LA, Hadaway L, Hagle ME, Broadhurst D, Clare S, Kleidon T, et al. Infusion Therapy Standards of Practice, 8th Edition. J Infus Nurs. 2021;44(1S Suppl 1):S1-S224.
- Duems-Noriega O, Arino-Blasco S. Subcutaneous fluid and drug delivery: safe, efficient and inexpensive. Reviews in Clinical Gerontology. 2015;25(2):117-46.
- Caccialanza R, Constans T, Cotogni P, Zaloga GP, Pontes-Arruda A. Subcutaneous Infusion of Fluids for Hydration or Nutrition: A Review. JPEN J Parenter Enteral Nutr. 2018;42(2):296-307.
- Gomes NS, Silva A, Zago LB, Silva E, Barichello E. Nursing knowledge and practices regarding subcutaneous fluid administration. Rev Bras Enferm. 2017;70(5):1096-105.
- Spandorfer PR, Mace SE, Okada PJ, Simon HK, Allen CH, Spiro DM, et al. A randomized clinical trial of recombinant human hyaluronidase-facilitated subcutaneous versus intravenous rehydration in mild to moderately dehydrated children in the emergency department. Clin Ther. 2012;34(11):2232-45.
- Good P, Richard R, Syrmis W, Jenkins-Marsh S, Stephens J. Medically assisted hydration for adult palliative care patients. Cochrane Database Syst Rev. 2014(4):CD006273.
- Forbat L, Kunicki N, Chapman M, Lovell C. How and why are subcutaneous fluids administered in an advanced illness population: a systematic review. J Clin Nurs. 2017;26(9-10):1204-16.
- Woodward M. Guidelines to effective hydration in aged care facilities 2013 15/02/2022.
- Vivanti A, Harvey K, Ash S, Battistutta D. Clinical assessment of dehydration in older people admitted to hospital: what are the strongest indicators? Arch Gerontol Geriatr. 2008;47(3):340-55.
- Hooper L, Abdelhamid A, Attreed NJ, Campbell WW, Channell AM, Chassagne P, et al. Clinical symptoms, signs and tests for identification of impending and current water-loss dehydration in older people. Cochrane Database Syst Rev. 2015(4):CD009647.
- Volkert D, Beck AM, Cederholm T, Cruz-Jentoft A, Goisser S, Hooper L, et al. ESPEN guideline on clinical nutrition and hydration in geriatrics. Clin Nutr. 2019;38(1):10-47.
- Group GE. Gastrointestinal. 2021. In: Rehydration in adults [Internet]. Melbourne: Therapeutic Guidelines Limited.
- Guidelines for Subcutaneous Infusion Device Management in Palliative care and other settings. In: Education CfPCRa, editor. 3 ed. Brisbane: Queensland Health; 2021.
- Vivanti AP. Origins for the estimations of water requirements in adults. Eur J Clin Nutr. 2012;66(12):1282-9.
- Vivanti AP, Campbell KL, Suter MS, Hannan-Jones MT, Hulcombe JA. Contribution of thickened drinks, food and enteral and parenteral fluids to fluid intake in hospitalised patients with dysphagia. J Hum Nutr Diet. 2009;22(2):148-55.
-
Pathway Dehydration and subcutaneous fluids Document ID CEQ-HIU-FRAIL-00012 Version no. 2.0.0 Approval date 06/06/2022 Executive sponsor Executive Director, Healthcare Improvement Unit Author Improving the quality and choice of care setting for residents of aged care facilities with acute healthcare needs steering committee Custodian Queensland Dementia Ageing and Frailty Network Supersedes 1.3.0 Applicable to Residential aged care facility (RACF) registered nurses and general practitioners in Queensland serviced by a RACF acute care Support Service (RaSS) Document source Internal (QHEPS) and external Authorisation Executive Director, Healthcare Improvement Unit Keywords Subcutaneous fluids, hypodermoclysis, dehydration Relevant standards Aged Care Quality Standards:
Standard 2: ongoing assessments and planning with consumers
Standard 3: personal care and clinical care, particularly 3(3)
Standard 8: organisational governance