Tracheostomy and laryngectomy emergencies
This information does not replace clinical judgement. Refer to Conditions of use and copyright for further T&Cs.
Residents with a tracheostomy or laryngectomy require rapid response to breathing difficulty - failure to ensure rapid, appropriate response is associated with high mortality. Rapid, appropriate response requires clinicians to be supported with appropriate training and have immediate access to required equipment.
All clinical staff providing care to residents with a tracheostomy or laryngectomy should familiarise themselves with this pathway prior to a requirement to implement it in an emergency setting.
Flowchart
The flowchart shows all of the information at one time. Health professionals should always remain within their scope of practice; these pathways should never replace clinical judgement.
Click the link below to view the full flowchart.
Practice points
The practice points are a systemised documentation of expanded relevant information - use only in conjunction with the flowchart - note, you can access each relevant point from the flowchart link.
-
Suspect a tracheostomy or laryngectomy emergency in a resident with a tracheostomy or laryngeal stoma who has any of the following symptoms or signs:
- Grunting, snoring or stridor.
- No evidence of breathing (apnoea).
- Increased work of breathing: accessory muscle use, increased respiratory rate, visible distress.
- New drop in oxygen saturations.
- Visibly displaced tracheostomy tube.
- Blood or blood-stained secretions around the tracheostomy tube.
- New onset anxiety, agitation and confusion.
-
Clinical assessment of breathing requires assessment at the mouth and nose and tracheostomy or stoma by:
Looking for:
- Tachypnoea (fast respiratory rate)
- Cyanosis (blue colour skin / mucous membranes) and reduced oxygen saturations
- Accessory muscle use
- Agitation / anxiety
- Reduced responsiveness
- Displaced tracheostomy tube or attachments
- Bleeding from around the tracheostomy tube
Listening for:
- Stridor or abnormal inspiratory noises suggesting a partially blocked or displaced tube
- Partial vocalisation: in a cuffed tube, this suggests an air leak around the cuff, which may indicate displacement or cuff leak
Feeling for:
- Movement of air in / out of mouth and nose and tracheostomy or stoma
-
A tracheostomy is a semi-permanent or permanent surgical opening to the trachea or main airway that allows the resident to breath via a tube. Although there is still an anatomical connection to the upper airways, the upper airway may be blocked as a result of swelling or a cancer.
A laryngectomy is the surgical removal of the larynx, with no connection from the nose or mouth to the lungs. Airway management using the upper airway (e.g. face-masks) will not work - the only airway that the patient has is the airway on the front of the neck.
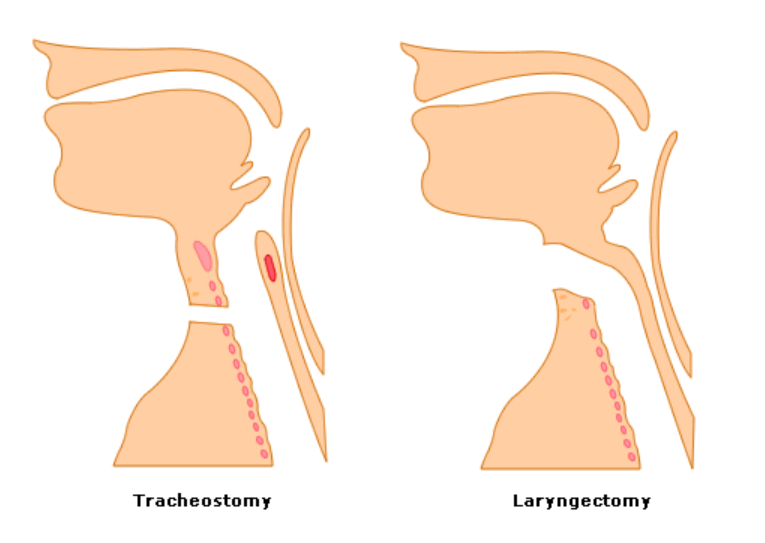
Image reproduced with permission from HEE eLfH.
-
Both tracheostomies or laryngectomy stomas may have attachments to support maintenance of a patent airway, speech, swallowing and humidification of inhaled air.
Tracheostomy attachments may include:
- An inner cannula or tube that sits inside the lumen of the tracheostomy tube (figure A shows the inner cannula removed and sitting beside the tracheostomy tube and figure B shows the inner cannula inserted within the tracheostomy tube). The inner cannula is designed to be removed and washed regularly.
Figure A: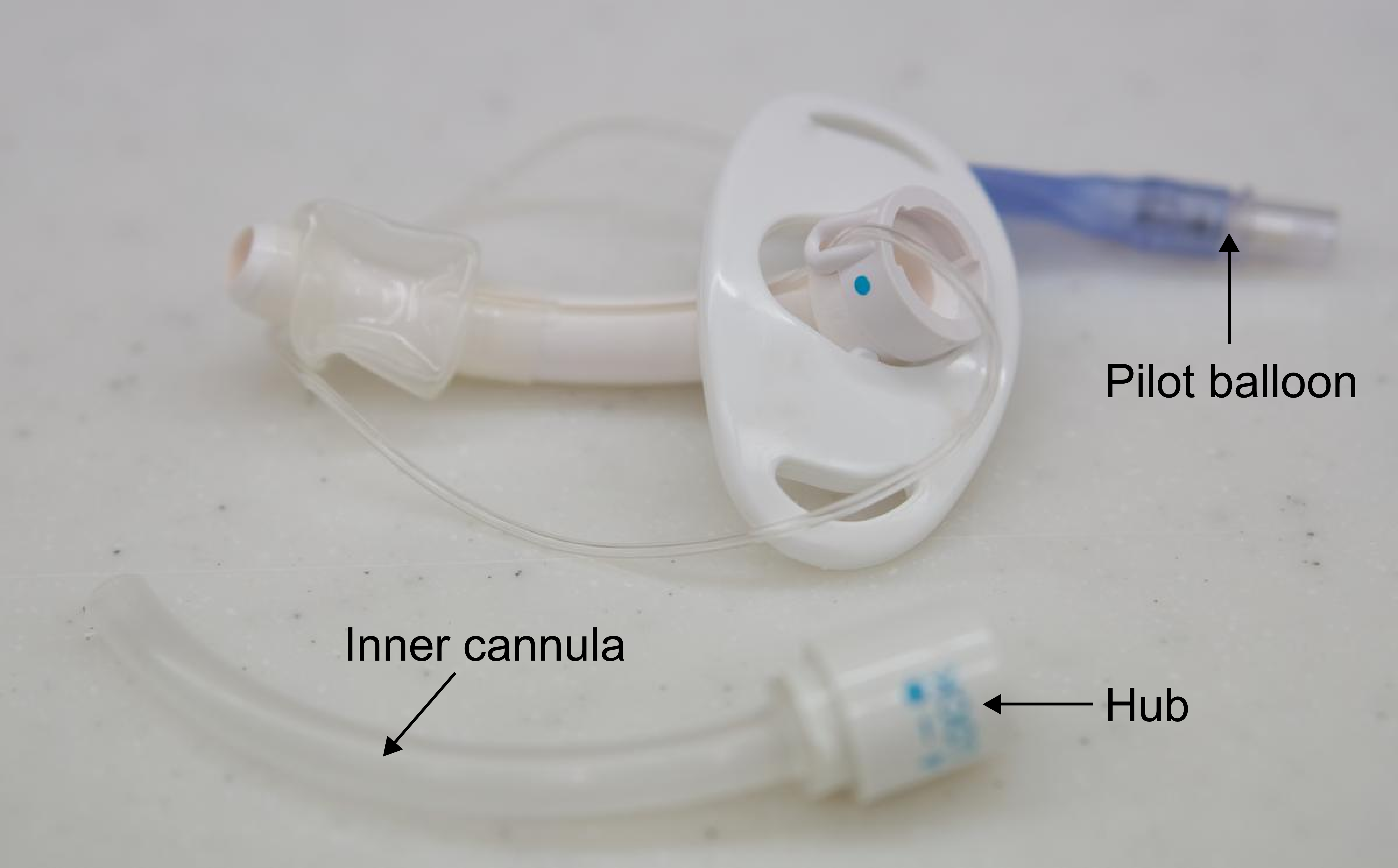
Shutterstock 355018688
Figure B: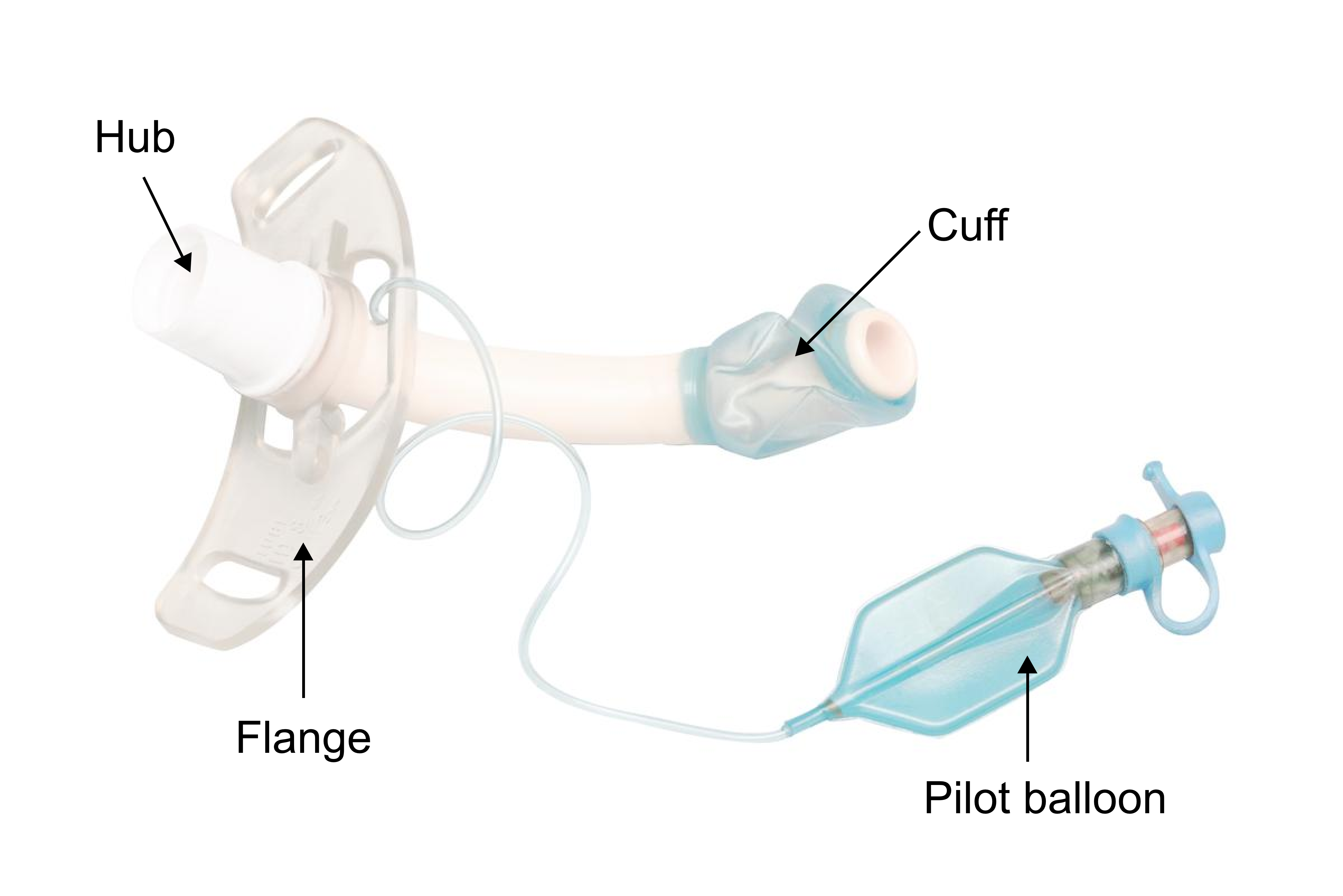
Shutterstock 1156851781 - A speaking valve or cap (see figure C below) is a device that connects to the hub of the tracheostomy tube and either allows airflow in but blocks airway out (speaking valve) or blocks airflow in or out (cap). In figure C, speaking valves speaking valves are marked "b" in the image, and a cap is marked "a".
Figure C: Speaking valves
Image reproduced with permission from the National Tracheostomy Safety Project - Humidification in a spontaneously breathing resident is usually via a Heat Moisture Exchanger (commonly a Swedish nose) - see figures C (item labelled "c") and figure D.
Figure D: Heat Moisture Exchanger (Swedish nose)
Image reproduced with permission from the National Tracheostomy Safety Project
Laryngectomy attachments may include:
A voice prosthesis (see figure E) - it is important to not remove the voice prosthesis when suctioning.
Figure E: Voice prosthesis
Image reproduced with permission from the National Tracheostomy Safety Project
- An inner cannula or tube that sits inside the lumen of the tracheostomy tube (figure A shows the inner cannula removed and sitting beside the tracheostomy tube and figure B shows the inner cannula inserted within the tracheostomy tube). The inner cannula is designed to be removed and washed regularly.
-
Suctioning a tracheostomy / laryngectomy should be performed by those skilled in the procedure as tracheal damage and hypoxia may occur due to poorly performed suction.
- Clinician has the required training and scope of practice.
- Prepare equipment:
- Suction catheter selection:
- selection of an appropriately sized suction catheter may minimise hypoxia (too large a catheter will occlude the tracheal tube)
- suction catheter external diameter should be no more than half the internal diameter of the tracheostomy tube
- Suction should be performed using a sterile technique, with the clinician performing hand hygiene and wearing appropriate Personal Protective Equipment
- Where oximetry is available, it is advised to monitor oxygen saturations during suctioning
- Suction catheter selection:
- Prepare the resident. Prior to suctioning ensure that:
- Vital signs have been performed and the intervention remains appropriate
- The procedure has been explained to the resident and the resident consents (where able)
- Resident has had oxygen applied and is positioned appropriately (supported sitting if able) and
- Speaking valve or cap has been removed and
- The inner cannula has been removed and cleaned and re-inserted
(** IMPORTANT: where the resident’s inner cannula is fenestrated, replace with a non-fenestrated
inner cannula prior to suctioning) - see figure F - The suction unit has been tested and is working and suction unit is set at no more than 120mmHg
Figure F: Fenestrated (top) and Non-fenestrated (bottom) inner cannulae

Image reproduced with permission from the National Tracheostomy Safety Project - Insert suction catheter via tracheostomy without suction activated until resistance is felt at the carina (usually ~ 15-20 cm).
- If the suction catheter is unable to be passed beyond the tracheostomy, the tracheostomy is not patent - deflate the tracheostomy cuff (where present) and look, listen and feel for breathing at the mouth and tracheostomy. If there is no improvement, remove the tracheostomy tube. Reapply oxygen to face and over tracheostomy tube or stoma. Refer to the pathway for further actions.
- Where the suction catheter is passed, withdraw the catheter 1 cm from the carina and then apply suction whilst withdrawing catheter with a rolling of the suction tubing between two fingers. Suction time from insertion to completion should not exceed 10 seconds.
-
Tracheostomy / laryngectomy day-to-day care should involve regular assessment of vital signs and escalating if any changes are noted. Frequency of vital signs should be individualised and guided by the resident's specialist treating teams and GP.
Additionally, residents with a tracheostomy / laryngectomy require the following daily care:
- Humidification - ensure appropriate humidification is provided, such as through a heat moisture exchange device (HME) or stoma bib. Refer to the recommendation of the resident’s specialist.
- Checks of bedside equipment (at least once daily) - this should include:
- Basic airway equipment including oxygen masks, self-inflating bag-valve-mask
- Oxygen cylinder with regulator
- Spare tracheostomy tubes (one the same size and one tube one size smaller)
- Clean pot for spare inner cannula
- Suction with selection of appropriate suction catheters
- Humidification equipment
- Sterile dressing pack and sterile lubricating jelly
- Scissors
- Tracheostomy dressings and securement tapes
- Personal protective equipment
- Sterile gloves
- Nurse call bell (resident may be unable to verbally call for help)
- Bedside equipment checklist
- Suctioning in residents unable to clear their own secretions. Staff should be trained and competent in providing suction to the tracheostomy and deep suctioning.
- Cleaning and replacement (or for disposable inner cannulae, changing) of the inner cannula.
- Checking and managing cuff pressure.
- Stoma care - check stoma site at least once a day. The site should be cleaned using a tracheostomy wipe or with 0.9% saline and dried thoroughly. Monitor for signs of infection including purulent exudate, redness, pain or swelling. A film-forming barrier, such as Cavilon Barrier Wipe, may protect the stoma site from wet secretions and may reduce risk of maceration of skin.
- Tracheostomy securement device - check once per shift (or more frequently if resident is at risk of pulling on the collar / ties) and prior to turning a resident in bed or performing pressure injury cares.
- Oral care - regular mouth care is essential in residents with a tracheostomy or laryngectomy.
- Communication with resident and treating specialist / GP of any concerns; ensuring that all clinical staff delivering care to the resident are aware of the resident’s tracheostomy / laryngectomy.
- Documentation of tracheostomy cares.
-
Facilities with residents with a tracheostomy / laryngectomy should ensure that there are established processes to facilitate:
- Hand-over to all clinical staff to ensure that daily cares for tracheostomy / laryngectomy are completed and documented.
- Regular training and competency of clinical staff in tracheostomy / laryngectomy cares and emergency response.
- Bedside emergency algorithms specific to the resident (including whether resident has a tracheostomy or laryngectomy and emergency algorithm aligned to resident’s goals of care).
- Processes to support regular daily checks of bedside equipment.
- Resident is linked in to appropriate specialist clinic to support regular review and clinical support.
- All residents with a tracheostomy or laryngectomy have access to regular speech therapy review and support.
References
-
- Everitt E. Caring for patients with a tracheostomy. Nurs Times. 2016;112(19):16-20.
- Mitchell RB, Hussey HM, Setzen G, Jacobs IN, Nussenbaum B, Dawson C, et al. Clinical consensus statement: tracheostomy care. Otolaryngol Head Neck Surg. 2013;148(1):6-20.
- National Tracheostomy Safety Project. Emergency tracheostomy management - patient upper airway. 2016. Available at: https://www.tracheostomy.org.uk/storage/files/Patent%20Airway%20Algorithm.pdf accessed 19/01/2023.
- National Tracheostomy Safety Project. Emergency laryngectomy management. 2020. https://www.tracheostomy.org.uk/storage/files/Laryngectomy%20Algorithm.pdf Accessed 19/01/2023.
- Graham JM, Fisher CM, Cameron TS, Streader TG, Warrillow SJ, Chao C, et al. Emergency tracheostomy management cognitive aid. Anaesth Intensive Care. 2021;49(3):227-31.
- McGrath BA, Bates L, Atkinson D, Moore JA, National Tracheostomy Safety P. Multidisciplinary guidelines for the management of tracheostomy and laryngectomy airway emergencies. Anaesthesia. 2012;67(9):1025-41.
- Long B, Koyfman A. Resuscitating the tracheostomy patient in the ED. Am J Emerg Med. 2016;34(6):1148-55.
- Bontempo LJ, Manning SL. Tracheostomy Emergencies. Emerg Med Clin North Am. 2019;37(1):109-19.
-
Pathway Tracheostomy / laryngectomy emergencies Document ID CEQ-HIU-FRAIL-00028 Version no. 2.0.0 Approval date 19/06/2023 Executive sponsor Executive Director, Healthcare Improvement Unit Author Improving the quality and choice of care setting for residents of aged care facilities with acute healthcare needs steering committee and Queensland Surgical Advisory Committee Custodian Queensland Dementia Ageing and Frailty Network Supersedes Tracheostomy v1.0 Applicable to Residential aged care facility registered nurses and General Practitioners in Queensland RACFs, serviced by a RACF acute care support service (RaSS) Document source Internal (QHEPS) and external Authorisation Executive Director, Healthcare Improvement Unit Keywords Tracheostomy, laryngectomy Relevant standards Aged Care Quality Standards:
Standard 2: ongoing assessments and planning with consumers
Standard 3: personal care and clinical care, particularly 3(3)
Standard 8: organisational governance